 Are You a Slow Caffeine Metabolizer?
Are You a Slow Caffeine Metabolizer?
Caffeine is a natural stimulant found in coffee beans, tea leaves, cacao pods, kola nuts, other plants, and synthetic sources of caffeine, including energy drinks, gum, snacks, and medications. Caffeine is known for its energy-boosting benefits. It may also help to support your cognition, mood, fat burning, exercise performance, gut health, and skin health and may also reduce your risk of disease. There may be some issues with caffeine, and not all people metabolize it the same. If you are a slow caffeine metabolizer, this article is for you.
In this article, you will learn about caffeine. I will discuss the benefits of caffeine and some potential problems with it. I will explain how your body metabolizes caffeine. I will go over the factors that may impact caffeine metabolism, including genetics. I will recommend some genetic testing that can help you figure out if you are a slow caffeine metabolizer. I will also offer my best tips for caffeine usage.
What is Caffeine
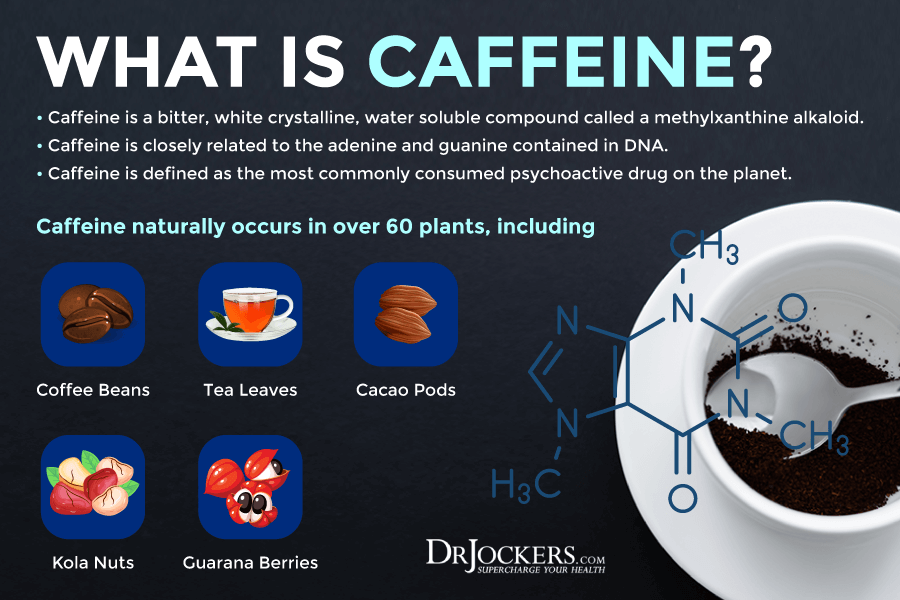
Caffeine is a bitter substance and natural stimulant. It naturally occurs in over 60 plants, including coffee beans, tea leaves, cacao pods, kola nuts, and guarana berries (1).
You can also find man-made or synthetic caffeine in some food and drinks, including energy drinks, gum, and snacks. There is also synthetic caffeine in certain cold medications, pain relief medication, over-the-counter (OCT) drugs for alertness, medication for menstrual cramps, and other medicines (1).
Caffeine is most commonly used for its ability to boost your energy and ‘wake you up’. It’s also a diuretic and can help to go to the bathroom. Caffeine offers several health benefits, but there are also some problems when it comes to your body’s ability to metabolize caffeine. Moderate consumption of is safe for most people. However, it can depend on your body and personal health (1).
How Caffeine Works:
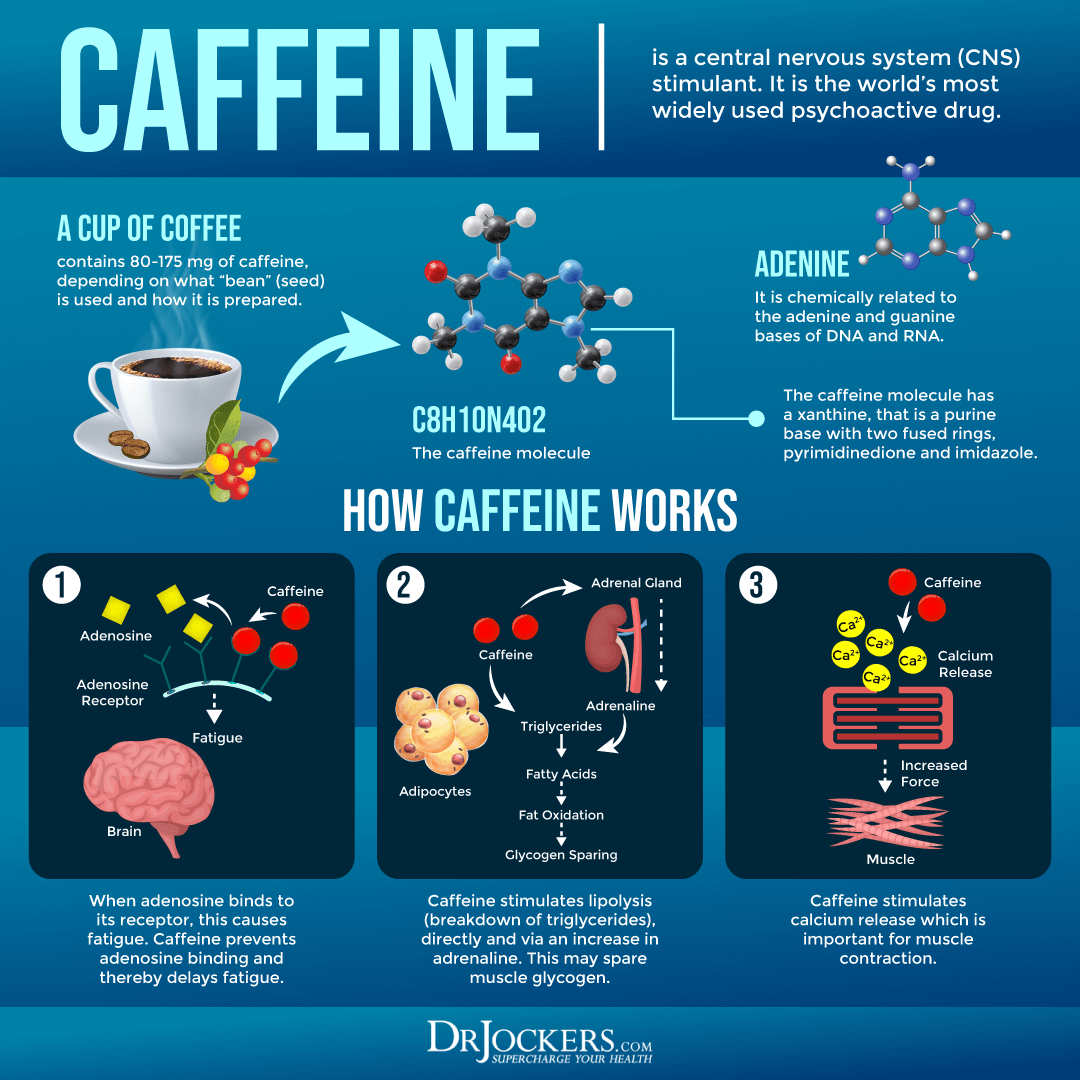
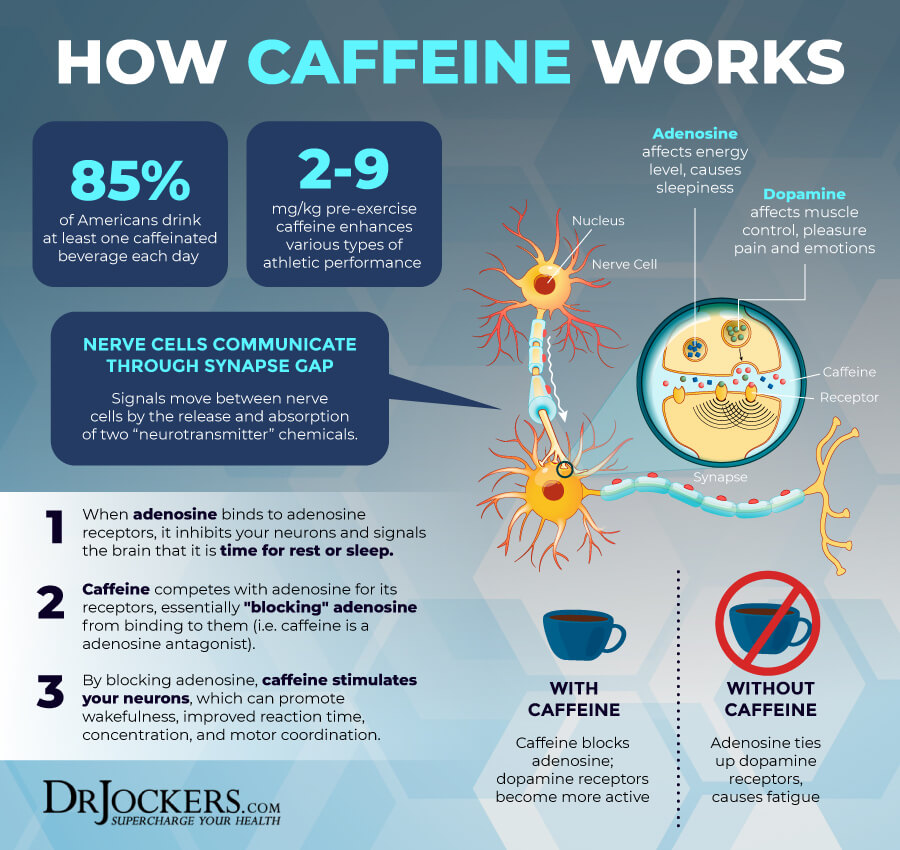
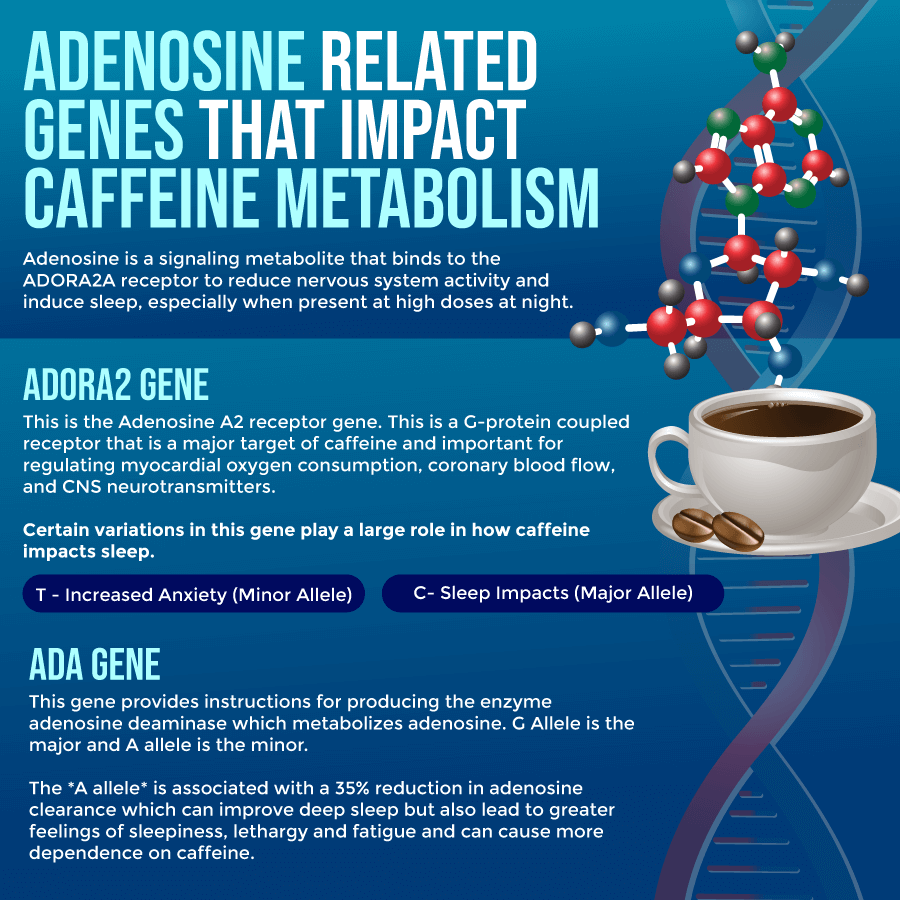
In our nervous system we have a signaling metabolite called adenosine that works to slow down the nervous system activity. When enough adenosine binds to adenosine receptors, it inhibits neuronal activity and signals to the brain that it is time to rest and sleep.
Caffeine works as an adenosine antagonist by competing with adenosine for its receptors and blocking adenosine from binding to its receptor. By blocking adenosine, caffeine stimulates the neurons, which promotes wakefulness, improved reaction time, concentration and motor coordination.
Benefits of Caffeine
Caffeine has several potential health benefits, including:
- Better mood and brain function: According to a 2010 study published in Food Science, caffeine may improve alertness, short-term memory, and reaction time (1). According to a 2010 article published in Molecular Nutrition and Food Research, it may improve mood and reduce the risk of depression (2).
- Improved metabolism and fat burning: According to a 2004 clinical trial published in the American Journal of Clinical Nutrition, caffeine may stimulate metabolism and energy expenditure (3). According to a 2012 study published in Obesity, it may boost calorie burning (4).
- Improved exercise performance: According to a 2013 study published in PLoS One, caffeine may help to improve endurance (5). According to a 2010 study published in Food Science, it may reduce fatigue and support muscle contractions (1).
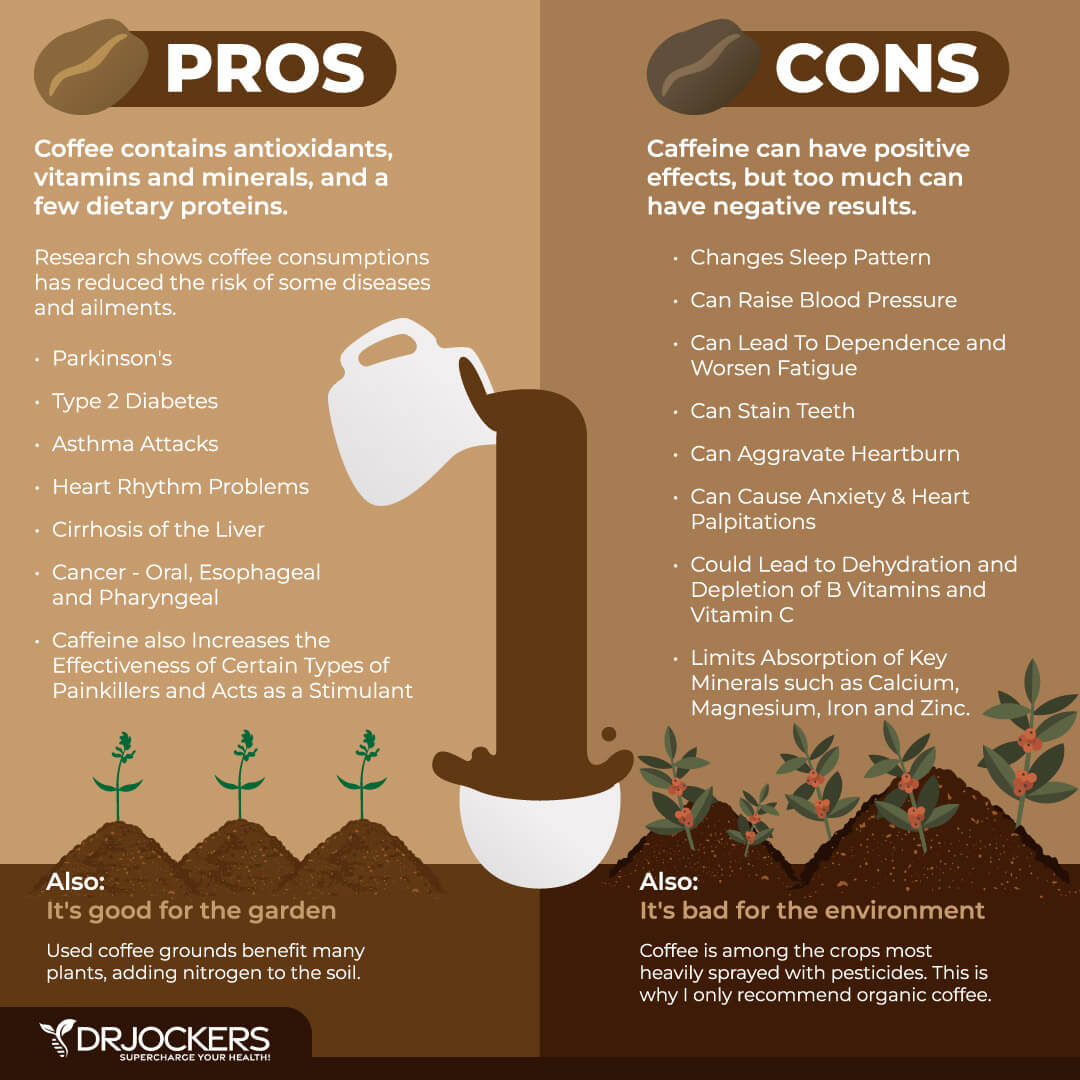
- Reduced risk of chronic diseases: According to a 2013 review published in the Journal of American College of Cardiology, caffeine may help to reduce the risk of cardiovascular and cardiometabolic disease and mortality (6). According to 2014 research published in the European Journal of Nutrition, caffeine may reduce the risk of type 2 diabetes (7). According to a 2013 review published in BMC Gastroenterology, it may help to reduce the risk of cancer (8).
- Improved gut health: According to a 2009 clinical trial published in the International Journal of Food Microbiology, caffeine may help to improve the gut microbiome (9). According to a 2020 study published in Nutrients, it may help to improve fecal microbial composition (10).
- Better skin health: According to a 2015 study published in the Journal of National Cancer Institute, caffeine may help to reduce the risk of melanoma (11). According to a 2016 review published in PLoS One, it may be linked to a reduced risk of melanoma (12).
Problems with Caffeine
Though caffeine may offer several health benefits, there may also be some problems, risks, and side effects when it comes to caffeine. According to a 2009 review published in Drug and Alcohol Dependence, excess caffeine intake may lead to tremors, irregular heartbeat, anxiety, and insomnia (13). Caffeine may also be addictive, and withdrawal can cause issues, including headaches, brain fog, and fatigue.
A 2004 study published in Neurology has also found that caffeine may lead to headaches or migraines (14). According to a 2009 review published in Pharmacology and Therapeutics, caffeine may also cause high blood pressure increasing cardiovascular risks (15). A 2014 review published in BMC Medicine has found that caffeine may not be right during pregnancy as it may increase the risk of low birth weight or miscarriage (16).
How the Body Metabolizes Caffeine
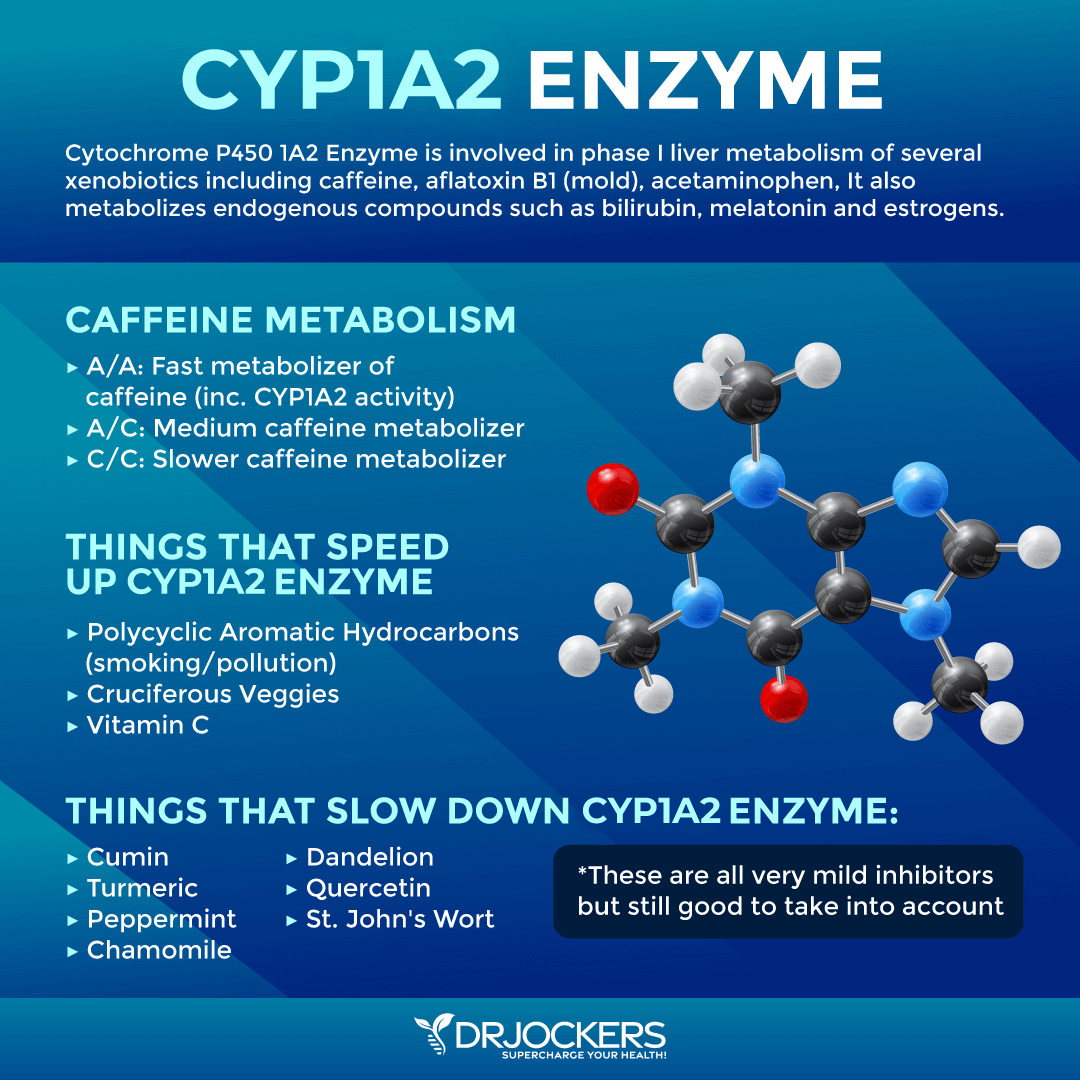
The cytochrome P450 enzymes are made by your liver. They are responsible for metabolizing caffeine. This enzyme is coded by the CYP1A2 gene. Variabilities of this gene can greatly influence the metabolism and clearance of caffeine. The C allele of CYP1A2 enzyme is associated with slower caffeine metabolism. This may also be influenced by genetic polymorphism, certain diseases, race, and gender (17, 18, 19).
A 1986 and a 2009 study both published in Clinical and Experimental Pharmacology and Physiology found that regular intake of caffeine does not change its pharmacokinetics (20, 21). However, a 2008 study published in the European Journal of Clinical Pharmacology has found that 3 cups of coffee a day may increase CYP1A2 activity (22).
Factors that Impact Caffeine Metabolism
There are several factors that may impact caffeine metabolism, including your liver health, smoking, alcohol, nutrition, pregnancy, oral contraceptives, medication, and genetics.
Liver Health
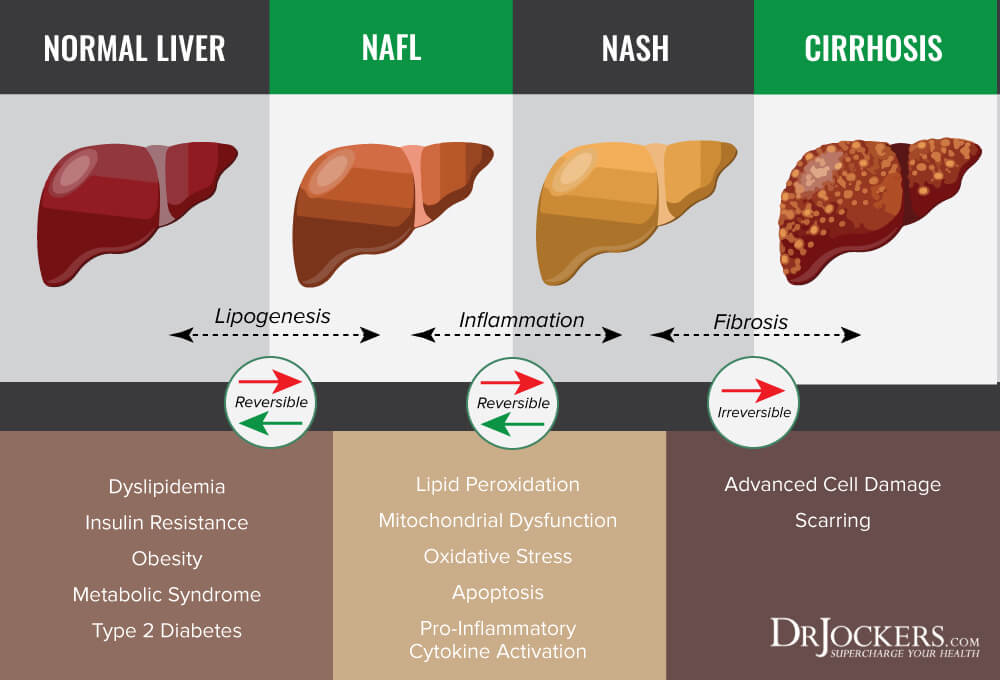
Your liver is responsible for caffeine metabolism. A 1980 study published in Digestive Diseases and Sciences has found that cirrhosis may impact caffeine metabolism and caffeine elimination (23). A 1988 study published in Clinical Sciences (London) has also found that chronic liver disease may lead to the reduction of plasma clearance of caffeine. (24).
A 2012 study published in Alimentary Pharmacology and Therapeutics has found that caffeine may actually be protective in those with non-alcoholic fatty liver disease (25). It seems that the impact of liver health on caffeine metabolism may depend on the progression of the disease and the amount of caffeine consumed.
Smoking and Alcohol
A 2018 review published in Pharmacology Reviews has found that smoking can stimulate and increase caffeine clearance due to enzyme induction (17). A 1988 study published in Clinical Pharmacology and Therapeutics has found that quitting smoking can reduce caffeine clearance and get the body back to normal caffeine metabolism (26).
According to a 1997 study published in Pharmacogenetics, alcohol can reduce CYP1A2 enzyme activity and impact caffeine clearance (27). A 1986 study published in Clinical and Experimental Pharmacology & Physiology has found that only 50 g of alcohol per day can decrease caffeine clearance to about half from 72 to 36 percent (20). According to a 2011 study published in Addiction, caffeine doesn’t improve the negative impact of alcohol intoxication, including impact (28).
Nutritional Habits
Nutritional habits can also affect your caffeine metabolism. According to a 1993 study published in the British Journal of Clinical Pharmacology and a 1995 study published in the International Journal of Clinical Pharmacology, grapefruit juice may decrease caffeine clearance (29, 30).
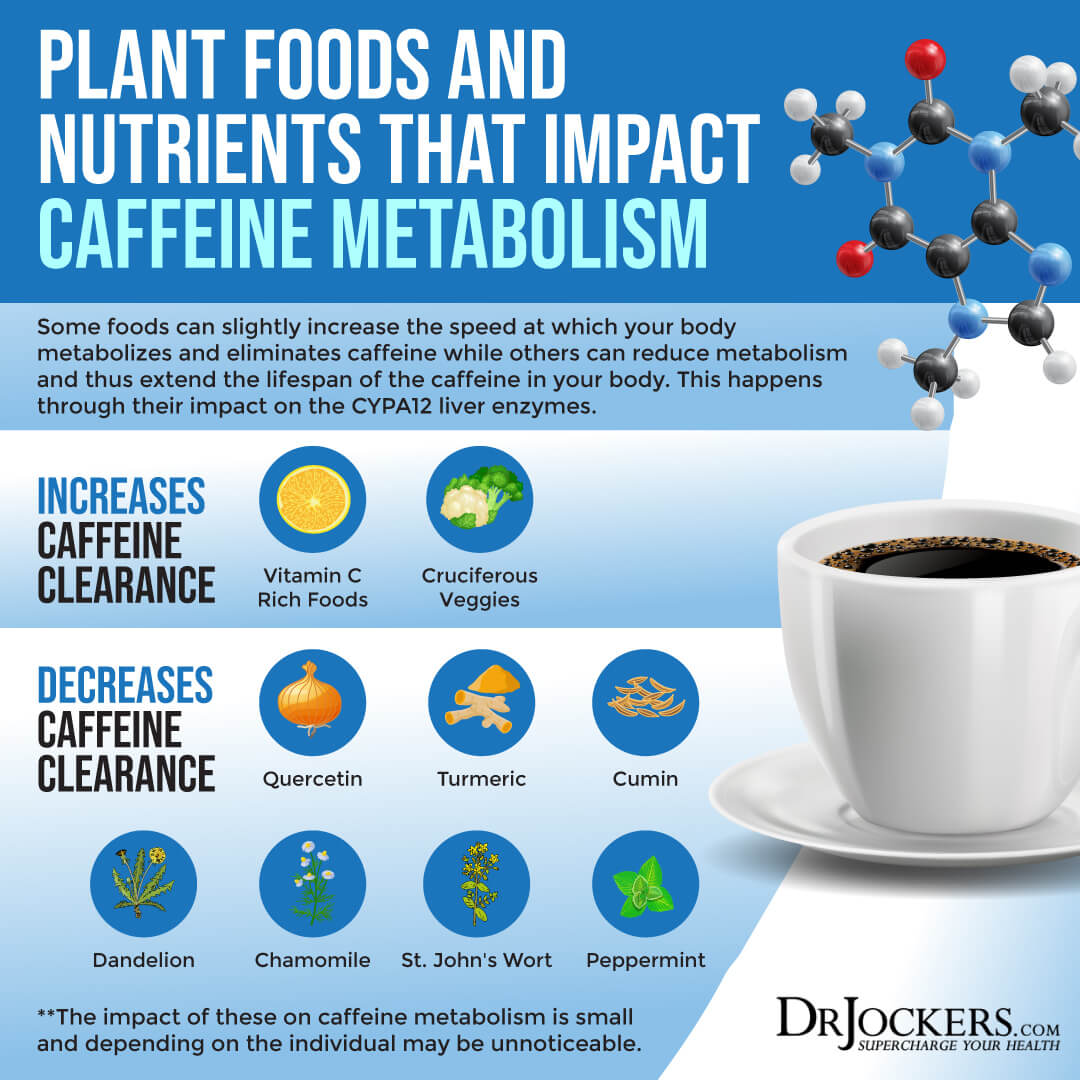
According to a 1984 journal article published by the Food and Agricultural Organization of the United States, vitamin C may also increase caffeine clearance (31). Although other research has said that vitamin C has very little impact on caffeine metabolism.
According to a 2009 study published in Xenobiotica, vegetables and fruits rich in flavonoids, such as quercetin, may also affect caffeine metabolism (32). Quercetin slows down CYP1A2 activity, extending the effects of caffeine in the body by reducing its metabolism and excretion.
Other herbs that may slightly decrease caffeine clearance include turmeric, cumin, dandelion, chamomile, St John’s wort and peppermint. Taking these herbs with caffeine may keep it in your system a bit longer by reducing CYPA12 metabolism and clearance.
Pregnancy
Pregnancy may also impact caffeine metabolism. A 1991 study published in the Journal of Pharmacology and Experimental Therapeutics and a 2016 study published in the Journal of Clinical Pharmacology has found that pregnancy may decrease caffeine metabolism, especially during the third trimester of the pregnancy (33, 34).
According to a 1993 book, Metabolism of Caffeine and Other Components of Coffee in Caffeine, Coffee, and Health, pregnancy may reduce enzyme activity related to caffeine metabolism and may increase its half-life (35). However, it seems that a few weeks after pregnancy, caffeine metabolism does return to normal.
According to the European Food Safety Authority (EFSA), published in 2015 in the EFSA Journal, the caffeine intake of pregnant women should be 200 mg or less in total, including any and all sources consumed that day (e.g., coffee, tea, chocolate) (36).
Oral Contraceptives
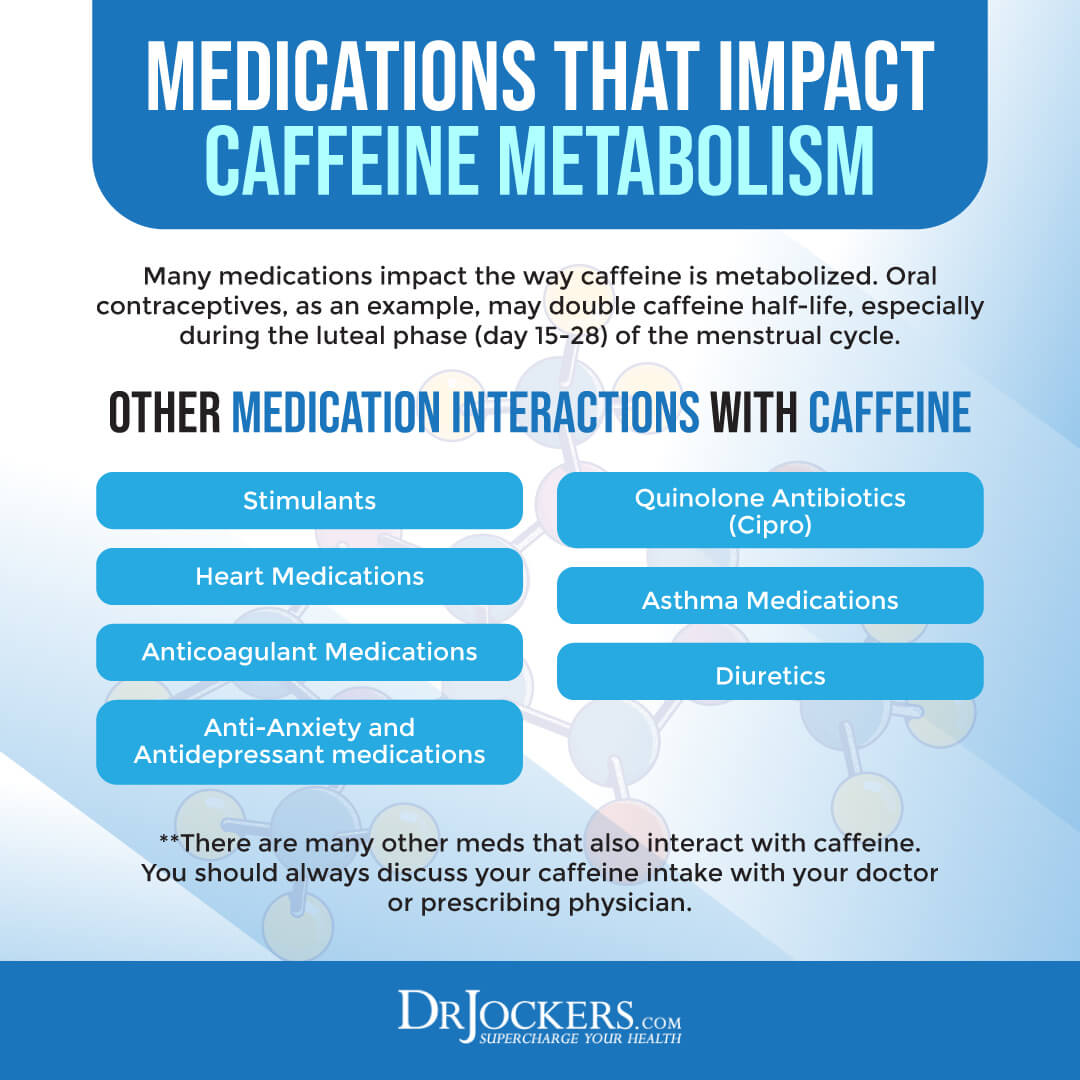
Using oral contraceptives may also influence caffeine metabolism. According to a 1993 book, Metabolism of Caffeine and Other Components of Coffee in Caffeine, Coffee, and Health, oral contraceptive use may double caffeine half-life, especially during the luteal phase of the menstrual cycle (35).
If you are on oral contraceptives, it is important to watch how your body responds to dosages of caffeine and modulate your dosages during the luteal phase of your menstrual cycle.
Medications
Some medications also affect caffeine pharmacokinetics and metabolism. A 2017 review published in Pharmacology Reviews has found that certain medications may interfere with caffeine metabolism (37).
This includes stimulant medications such as ephedrine, diuretics, asthma drugs and heart medications such as adenosine, dipyridamole and anti-coagulant meds. Additionally, thyroid medications, anti-depressants and quinolone antibiotics such as the commonly prescribed Cipro will interfere with caffeine metabolism.
The person’s caffeine intake should always be considered when prescribing and recommending the dosage of such medicines. Taking these medicines may require reducing or eliminating other sources of caffeine.
Genetic Variabilities
According to a 2010 study published in Pharmacology and a 2017 review published in Pharmacology Reviews, genetics and genetic polymorphisms may play a role in caffeine metabolism (37, 38).
The CYP1A2 gene is a protein coding gene. It is responsible for coding the cytochrome P450 enzyme, which is an enzyme made by your liver to metabolize caffeine. Genetic variabilities of the CYP1A2 gene may influence caffeine clearance and metabolism. (17, 18, 19).
According to a 2012 study published in Human Molecular Genetics, certain variants of CYP1A2 are linked to high caffeine intake. The combination of these variants and high caffeine intake may also reduce the risk of non-smokers from hypertension (39). According to a 2011 study published in Human Molecular Genetics, sequence variants of the CYP1A2 gene may affect coffee consumption and may explain the hereditary role of higher coffee consumption in certain cultures (40).
A 2007 study published in Cancer Epidemiology, Biomarkers & Prevention has found that CYP1A2 variation combined with coffee consumption may decrease the risk of breast cancer (41). According to 2016 research published in Clinical Pharmacology and Therapeutics, environmental effects, including smoking and oral contraceptives, may have genetic effects on the CYP1A2 activity (42).
According to a 2019 study published in Science Reports, the CYP1A2 and the ADORA2 genetic variations may both affect caffeine metabolism and caffeine’s effects on postprandial glycemia (43). The Adenosine A2 receptors are key for caffeine stimulation and metabolism. Having an ADORA2A genotype may increase the likelihood that someone is not as sensitive to caffeine. Thus, their caffeine consumption may also be naturally lower.
According to a 2012 study published in AJCN, caffeine may affect blood pressure, but there is variability in blood pressure response (44). Researchers found that genetic polymorphism of the adenosine A2A and α2-adrenergic receptors may be the cause of this variability. According to a 2011 study published in the European Journal of Neurology, the risk of Parkinson’s disease may be linked to ADORA2 polymorphism, which may or may not interact with coffee consumption (45).
A 2007 study published in Clinical Pharmacology and Therapeutics has found that the adenosine A2A receptor gene may vary in people with lower caffeine sensitivity and lower sleep quality (46). Thus, consuming the same amount of caffeine may impact different individuals differently depending on their genetic make-up.
Best Tips for Caffeine Usage
If you like coffee, tea, or other caffeine containing foods and beverages, I have a few tips for caffeine usage for maximum benefits:
- Drink caffeine 90 minutes after waking: When you wake up, your cortisol levels are naturally high, and adding caffeine to the mix may not be ideal. The benefits may be fewer, and you may also build up a tolerance easier. Using caffeine about 90 minutes after waking when your cortisol levels are lower, may help with an energy boost.
- Drink caffeine before your workout: Using caffeine 40 to 60 minutes before your workout may benefit you. It may help to increase energy support for your workout and improve fat oxidation. However, some people experience digestive issues from caffeine, especially coffee. If this is the case, you may want to reduce your dose, use it earlier, or skip it altogether.
- Add a pinch of salt to coffee: Coffee is a diuretic that can dehydrate your body and reduce electrolytes. Adding a pinch of Himalayan or Celtic sea salt to your coffee or under your tongue before drinking it may reduce this effect.
- Add some healthy fats: If your choice of caffeine is coffee, add some healthy fats. Coffee may help digestion, blood sugar levels, and fat loss. Adding some C8 MCT oil to your coffee may help to improve nutritional ketosis and fat loss.
- Consider magnesium: Caffeine itself may help to improve cognition, memory, and learning. Adding some magnesium to the mix can further improve your concentration and focus. I recommend using 1 to 2 scoops of Unsweetened Brain Calm Magnesium. You may mix it into your coffee, add it to a shake, or drink it as is.
- Start slow: If you are a slow caffeine metabolizer, use a smaller amount. Start with 40 to 50 mg of caffeine. This is about ½ cup of coffee. See how you feel, and if you feel good, you may increase your dose. Listen to your body.

Use an Organic, Mycotoxin Free, Shade Grown Coffee
Many people respond very well to a moderate dose of caffeine on a regular basis, but they are consuming low quality conventional coffee and chemically laden energy drinks. These products contain pesticides, chemicals and mycotoxins that can be harmful to your health (47, 48, 49). It is important that you drink high-quality, organic, mycotoxin-free, and shade-grown coffee for optimal benefits and safety.
I personally love and highly recommend Lifeboost Coffee. This coffee is organic, free from GMO, shade-grown, sun-dried, pesticide and chemical-free, full of antioxidants, stomach-friendly, less acidic than most coffee, and fairly traded with a 2-year shelf life. Most importantly, it is absolutely delicious.
Final Thoughts
Caffeine is a natural stimulant found in coffee beans, tea leaves, cacao pods, kola nuts, other plants, and synthetic sources, including energy drinks, gum, snacks, and medications. Caffeine has many health benefits and some potential drawbacks. Not everyone metabolizes caffeine the same.
Thus, not everyone experiences the same effects from the same amount of the substance. I recommend that you try the genetic test I recommend for figuring out if you are a slow caffeine metabolizer and follow my best tips for caffeine usage.
If you want to work with a functional health coach, I recommend this article with tips on how to find a great coach. On our website, we offer long-distance functional health coaching programs. For further support with your health goals, just reach out—our fantastic coaches are here to support your journey.

Inflammation Crushing Ebundle
The Inflammation Crushing Ebundle is designed to help you improve your brain, liver, immune system and discover the healing strategies, foods and recipes to burn fat, reduce inflammation and Thrive in Life!
As a doctor of natural medicine, I have spent the past 20 years studying the best healing strategies and worked with hundreds of coaching clients, helping them overcome chronic health conditions and optimize their overall health.
In our Inflammation Crushing Ebundle, I have put together my very best strategies to reduce inflammation and optimize your healing potential. Take a look at what you will get inside these valuable guides below!
Sources in This Article Include:
1. Caffeine. Food Science. Link Here
2. Molecular nutrition and food research. 2010. Link Here
3. Acheson KJ, Gremaud G, Meirim I, Montigon F, Krebs Y, Fay LB, Gay LJ, Schneiter P, Schindler C, Tappy L. Metabolic effects of caffeine in humans: lipid oxidation or futile cycling? Am J Clin Nutr. 2004 Jan;79(1):40-6. doi: 10.1093/ajcn/79.1.40. PMID: 14684395
4. Effect of thermogenic beverage. Obesity. 2012 Link Here
5. Hodgson AB, Randell RK, Jeukendrup AE. The metabolic and performance effects of caffeine compared to coffee during endurance exercise. PLoS One. 2013;8(4):e59561. doi: 10.1371/journal.pone.0059561. Epub 2013 Apr 3. PMID: 23573201
6. O’Keefe JH, Bhatti SK, Patil HR, DiNicolantonio JJ, Lucan SC, Lavie CJ. Effects of habitual coffee consumption on cardiometabolic disease, cardiovascular health, and all-cause mortality. J Am Coll Cardiol. 2013 Sep 17;62(12):1043-1051. doi: 10.1016/j.jacc.2013.06.035. Epub 2013 Jul 17. PMID: 23871889
7. Jiang, X., Zhang, D. & Jiang, W. Coffee and caffeine intake and incidence of type 2 diabetes mellitus: a meta-analysis of prospective studies. Eur J Nutr 53, 25–38 (2014). Link Here
8. Sang, LX., Chang, B., Li, XH. et al. Consumption of coffee associated with reduced risk of liver cancer: a meta-analysis. BMC Gastroenterol 13, 34 (2013). Link Here
9. Jaquet M, Rochat I, Moulin J, Cavin C, Bibiloni R. Impact of coffee consumption on the gut microbiota: a human volunteer study. Int J Food Microbiol. 2009 Mar 31;130(2):117-21. doi: 10.1016/j.ijfoodmicro.2009.01.011. Epub 2009 Jan 23. PMID: 19217682
10. González S, Salazar N, Ruiz-Saavedra S, Gómez-Martín M, de Los Reyes-Gavilán CG, Gueimonde M. Long-Term Coffee Consumption is Associated with Fecal Microbial Composition in Humans. Nutrients. 2020 May 1;12(5):1287. doi: 10.3390/nu12051287. PMID: 32369976
11. Loftfield E, Freedman ND, Graubard BI, Hollenbeck AR, Shebl FM, Mayne ST, Sinha R. Coffee drinking and cutaneous melanoma risk in the NIH-AARP diet and health study. J Natl Cancer Inst. 2015 Jan 20;107(2):dju421. doi: 10.1093/jnci/dju421. PMID: 25604135
12. Liu J, Shen B, Shi M, Cai J. Higher Caffeinated Coffee Intake Is Associated with Reduced Malignant Melanoma Risk: A Meta-Analysis Study. PLoS One. 2016 Jan 27;11(1):e0147056. doi: 10.1371/journal.pone.0147056. PMID: 26816289
13. Reissig CJ, Strain EC, Griffiths RR. Caffeinated energy drinks–a growing problem. Drug Alcohol Depend. 2009 Jan 1;99(1-3):1-10. doi: 10.1016/j.drugalcdep.2008.08.001. Epub 2008 Sep 21. PMID: 18809264
14. 2004 Neurology. Link Here
15. Riksen NP, Rongen GA, Smits P. Acute and long-term cardiovascular effects of coffee: implications for coronary heart disease. Pharmacol Ther. 2009 Feb;121(2):185-91. doi: 10.1016/j.pharmthera.2008.10.006. Epub 2008 Nov 11. PMID: 19049813
16. Chen, LW., Wu, Y., Neelakantan, N. et al. Maternal caffeine intake during pregnancy is associated with risk of low birth weight: a systematic review and dose-response meta-analysis. BMC Med 12, 174 (2014).
17. Nehlig A. Interindividual Differences in_Caffeine Metabolism and Factors Driving Caffeine Consumption. Pharmacol Rev. 2018 Apr;70(2):384-411. doi: 10.1124/pr.117.014407. Epub 2018 Mar 7. PMID: 29514871
18. Yang A, Palmer AA, de Wit H. Genetics of_caffeine consumption and responses to caffeine. Psychopharmacology (Berl). 2010 Aug;211(3):245-57. doi: 10.1007/s00213-010-1900-1. Epub 2010 Jun 9. PMID: 20532872
19. Arnaud MJ. Pharmacokinetics and metabolism of natural methylxanthines in animal and man. Handb Exp Pharmacol. 2011;(200):33-91. doi: 10.1007/978-3-642-13443-2_3. PMID: 20859793
20. George J, Murphy T, Roberts R, Cooksley WG, Halliday JW, Powell LW. Influence of alcohol and caffeine_consumption on caffeine elimination. Clin Exp Pharmacol Physiol. 1986 Oct;13(10):731-6. doi: 10.1111/j.1440-1681.1986.tb02414.x. PMID: 3802578
21. Chen Y, Xiao P, Ou-Yang DS, Fan L, Guo D, Wang YN, Han Y, Tu JH, Zhou G, Huang YF, Zhou HH. Simultaneous action of the flavonoid quercetin on cytochrome P450 (CYP) 1A2, CYP2A6, N-acetyltransferase and xanthine oxidase activity in healthy volunteers. Clin Exp Pharmacol Physiol. 2009 Aug;36(8):828-33. doi: 10.1111/j.1440-1681.2009.05158.x. Epub 2009 Feb 10. PMID: 19215233
22. Djordjevic N, Ghotbi R, Bertilsson L, Jankovic S, Aklillu E. Induction of CYP1A2 by heavy coffee consumption in Serbs and Swedes. Eur J Clin Pharmacol. 2008 Apr;64(4):381-5. doi: 10.1007/s00228-007-0438-6. Epub 2007 Dec 22. PMID: 18157525
23. Desmond PV, Patwardhan RV, Johnson RF, Schenker S. Impaired elimination of caffeine in cirrhosis. Dig Dis Sci. 1980 Mar;25(3):193-7. doi: 10.1007/BF01308138. PMID: 7371463
24. Scott NR, Stambuk D, Chakraborty J, Marks V, Morgan MY. Caffeine_clearance and biotransformation in patients with chronic liver disease. Clin Sci (Lond). 1988 Apr;74(4):377-84. doi: 10.1042/cs0740377. PMID: 3356110
25. Birerdinc A, Stepanova M, Pawloski L, Younossi ZM. Caffeine_is protective in patients with non-alcoholic fatty liver disease. Aliment Pharmacol Ther. 2012 Jan;35(1):76-82. doi: 10.1111/j.1365-2036.2011.04916.x. Epub 2011 Nov 7. PMID: 22059453
26. Brown CR, Jacob P 3rd, Wilson M, Benowitz NL. Changes in rate and pattern of caffeine_metabolism after cigarette abstinence. Clin Pharmacol Ther. 1988 May;43(5):488-91. doi: 10.1038/clpt.1988.63. PMID: 3365914
27. Le Marchand L, Franke AA, Custer L, Wilkens LR, Cooney RV. Lifestyle and nutritional correlates of cytochrome CYP1A2 activity: inverse associations with plasma lutein and alpha-tocopherol. Pharmacogenetics. 1997 Feb;7(1):11-9. doi: 10.1097/00008571-199702000-00002. PMID: 9110357
28. Howland J, Rohsenow DJ, Arnedt JT, Bliss CA, Hunt SK, Calise TV, Heeren T, Winter M, Littlefield C, Gottlieb DJ. The acute effects of caffeinated versus non-caffeinated alcoholic beverage on driving performance and attention/reaction time. Addiction. 2011 Feb;106(2):335-41. doi: 10.1111/j.1360-0443.2010.03219.x. Epub 2010 Dec 6. PMID: 21134017
29. Fuhr U, Klittich K, Staib AH. Inhibitory effect of grapefruit juice and its bitter principal, naringenin, on CYP1A2 dependent metabolism of caffeine_in man. Br J Clin Pharmacol. 1993 Apr;35(4):431-6. doi: 10.1111/j.1365-2125.1993.tb04162.x. PMID: 8485024
30. Fuhr U, Maier A, Keller A, Steinijans VW, Sauter R, Staib AH. Lacking effect of grapefruit juice on theophylline pharmacokinetics. Int J Clin Pharmacol Ther. 1995 Jun;33(6):311-4. PMID: 7582380
31. AGRIS. 1984 Link Here
32. Chen Y, Tu JH, He YJ, Zhang W, Wang G, Tan ZR, Zhou G, Fan L, Zhou HH. Effect of sodium tanshinone II A sulfonate on the activity of CYP1A2 in healthy volunteers. Xenobiotica. 2009 Jul;39(7):508-13. doi: 10.1080/00498250902951763. PMID: 19534587
33. Bologa M, Tang B, Klein J, Tesoro A, Koren G. Pregnancy-induced changes in drug metabolism in epileptic women. J Pharmacol Exp Ther. 1991 May;257(2):735-40. PMID: 2033516
34. Yu T, Campbell SC, Stockmann C, Tak C, Schoen K, Clark EA, Varner MW, Spigarelli MG, Sherwin CM. Pregnancy-induced changes in the pharmacokinetics of caffeine and its metabolites. J Clin Pharmacol. 2016 May;56(5):590-6. doi: 10.1002/jcph.632. Epub 2015 Dec 22. PMID: 26358647
35. Arnaud M.J. (1993): Metabolism of caffeine_and other components of coffee, in_Caffeine, Coffee and Health (Garattini S ed), pp 43–95. Link Here
36. EFSA (2015): Scientific Opinion on the Safety of_Caffeine, EFSA Journal, 13(5):4102. Link Here
37. Nehlig A. (2017): Interindividual differences in caffeine_metabolism and factors driving caffeine consumption. Pharmacol Rev, 70(2):384-411. Link Here
38. Yang A. et al. (2010): Genetics of caffeine_consumption and responses to_caffeine. Psychopharmacol, 211(3):245-257. Link Here
39. Idris Guessous, Maria Dobrinas, Zoltán Kutalik, Menno Pruijm, Georg Ehret, Marc Maillard, Sven Bergmann, Jacques S. Beckmann, Daniele Cusi, Federica Rizzi, Franco Cappuccio, Jacques Cornuz, Fred Paccaud, Vincent Mooser, Jean-Michel Gaspoz, Gérard Waeber, Michel Burnier, Peter Vollenweider, Chin B Eap, Murielle Bochud, Caffeine intake and CYP1A2 variants associated with high_caffeine intake protect non-smokers from hypertension, Human Molecular Genetics, Volume 21, Issue 14, 15 July 2012, Pages 3283–3292, Link Here
40. Patrick Sulem, Daniel F. Gudbjartsson, Frank Geller, Inga Prokopenko, Bjarke Feenstra, Katja K.H. Aben, Barbara Franke, Martin den Heijer, Peter Kovacs, Michael Stumvoll, Reedik Mägi, Lisa R. Yanek, Lewis C. Becker, Heather A. Boyd, Simon N. Stacey, G. Bragi Walters, Adalbjorg Jonasdottir, Gudmar Thorleifsson, Hilma Holm, Sigurjon A. Gudjonsson, Thorunn Rafnar, Gyda Björnsdottir, Diane M. Becker, Mads Melbye, Augustine Kong, Anke Tönjes, Thorgeir Thorgeirsson, Unnur Thorsteinsdottir, Lambertus A. Kiemeney, Kari Stefansson, Sequence variants at CYP1A1–CYP1A2 and AHR associate with coffee consumption, Human Molecular Genetics, Volume 20, Issue 10, 15 May 2011, Pages 2071–2077, Link Here
41. The CYP1A2 Genotype Modifies the Association Between Coffee Consumption and Breast Cancer Risk Among BRCA1 Mutation Carriers. Cancer Epidemiol Biomarkers Prev (2007) 16 (5): 912–916. Link Here
42. Matthei J. Heritability of Caffeine_Metabolism: Environmental Effects Masking Genetic Effects on CYP1A2 Activity but Not on NAT2. 2016 Link Here
43. Banks, N.F., Tomko, P.M., Colquhoun, R.J. et al. Genetic Polymorphisms in ADORA2A and CYP1A2 Influence Caffeine’s Effect on Postprandial Glycaemia. Sci Rep 9, 10532 (2019). Link Here
44. Renda G. et al. (2012): Genetic determinants of blood pressure responses to caffeine_drinking. AJCN, 95(1):241-248. Link Here
45. Popat R.A. et al. (2011): Coffee, ADORA2A, and CYP1A2: the caffeine connection in Parkinson’s disease. Eur J Neurol, 18:756-765. Link Here
46. Retey J.V. et al. (2007): A genetic variation in the adenosine A2A receptor gene (ADORA2A) contributes to individual sensitivity to caffeine effects on sleep. Clin Pharmacol Ther, 81:692–8. Link Here
47. Sakamoto K, Nishizawa H, Manabe N. [Behavior of pesticides in coffee beans during the roasting process]. Shokuhin Eiseigaku Zasshi. 2012;53(5):233-6. Japanese. doi: 10.3358/shokueishi.53.233. PMID: 23154763
48. Martins ML, Martins HM, Gimeno A. Incidence of microflora and of ochratoxin A in green coffee beans (Coffea arabica). Food Addit Contam. 2003 Dec;20(12):1127-31. doi: 10.1080/02652030310001620405. PMID: 14726276
49. Studer-Rohr I, Dietrich DR, Schlatter J, Schlatter C. The occurrence of ochratoxin A in coffee. Food Chem Toxicol. 1995 May;33(5):341-55. doi: 10.1016/0278-6915(94)00150-m. PMID: 7759018

Good morning Dr Jockers (from Spain)
I would like to congratulate you because it is one of the best articles I have ever read about coffee.
Thank you for your work, helping others with honesty
Thank you for all your support Pascual! Blessings to you!