 DUTCH Test: Analyzing Hormone Levels for Optimal Health
DUTCH Test: Analyzing Hormone Levels for Optimal Health
The Dutch test is a comprehensive hormone test and the results are tested through dried urine. DUTCH is an acronym and stands for Dried Urine Test for Complete Hormones. This test is one of the most comprehensive hormone tests because it is a complete test of sex and adrenal hormones.
Many people are dealing with symptoms associated with stress and hormonal imbalances. These include things like depression, anxiety, fatigue, irregular periods, premenstrual syndrome, menopausal issues, low libido, erectile dysfunction, hair thinning, dry skin, hot flashes, fibrocystic breasts and more.
The mainstream medical testing offers little answers when it comes to these problems. Fortunately, the detailed stress hormone and sex hormone metabolites the DUTCH analysis provides give a great window into how the body is responding to stress and producing and metabolizing hormones.
This data can provide real answers as to root cause factors for a wide variety of health challenges. Even your risk for certain hormonal influenced cancers such as breast, uterine, endometrial, colon and prostate all have metabolic features that can be assessed through a detailed hormonal screening as well. In this article, we will discuss the details on the DUTCH and give you an understanding of how to interpret much of the findings.
What Does This Test Measure?
Precision Analytical labs developed this unique test. It measures your hormone metabolites from dried urine samples. The hormones include:
- Cortisol
- Cortisone
- Estradiol
- Estrone
- Estriol
- Progesterone
- Testosterone
- DHEA
- Melatonin
This test also measures your cortisol and cortisone rhythms and levels, and your estrogen metabolism pathways.
Additionally, it looks at 8-OHdG which is a marker of oxidative stress and it looks at several key neurotransmitter metabolites that view dopamine, norepinephrine and serotonin production. It also looks at several markers for B vitamin status.
Who Can Get Tested:
Any human, both male and female, who are wanting one of the most comprehensive analysis of their hormones can get this test run by a health care coach or provider. It does not matter if a woman is pre or post-menopausal taking birth control, hormone replacement therapy.
If a patient is pre-menopausal, the ideal time for collecting the samples is during the luteal phase between days 19 and 22 of a 28 day cycle. If someone is not on a cycle, they can get their hormones tested at any time. 4 to 5 samples are taken over a 24 hour period, the samples are allowed to dried and then sent in for analysis.
If you are interested in ordering this lab, you can get it from us here and one of our well trained team members will help you understand the results.

Why The DUTCH Test
Precision Analytical pride themselves on relentlessly pursuing the most accurate and precise techniques available for testing hormones and their metabolites. Why is it better than other types of hormone tests?
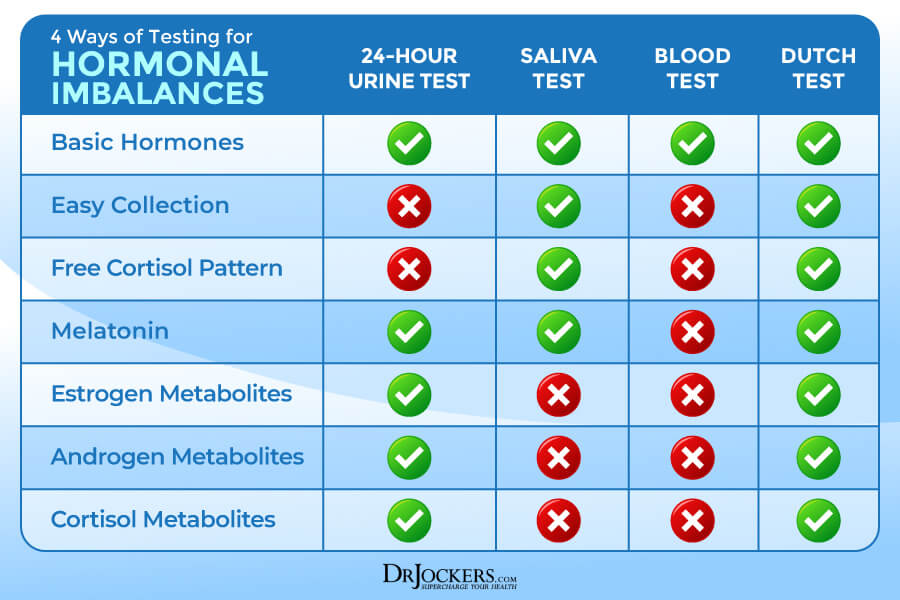
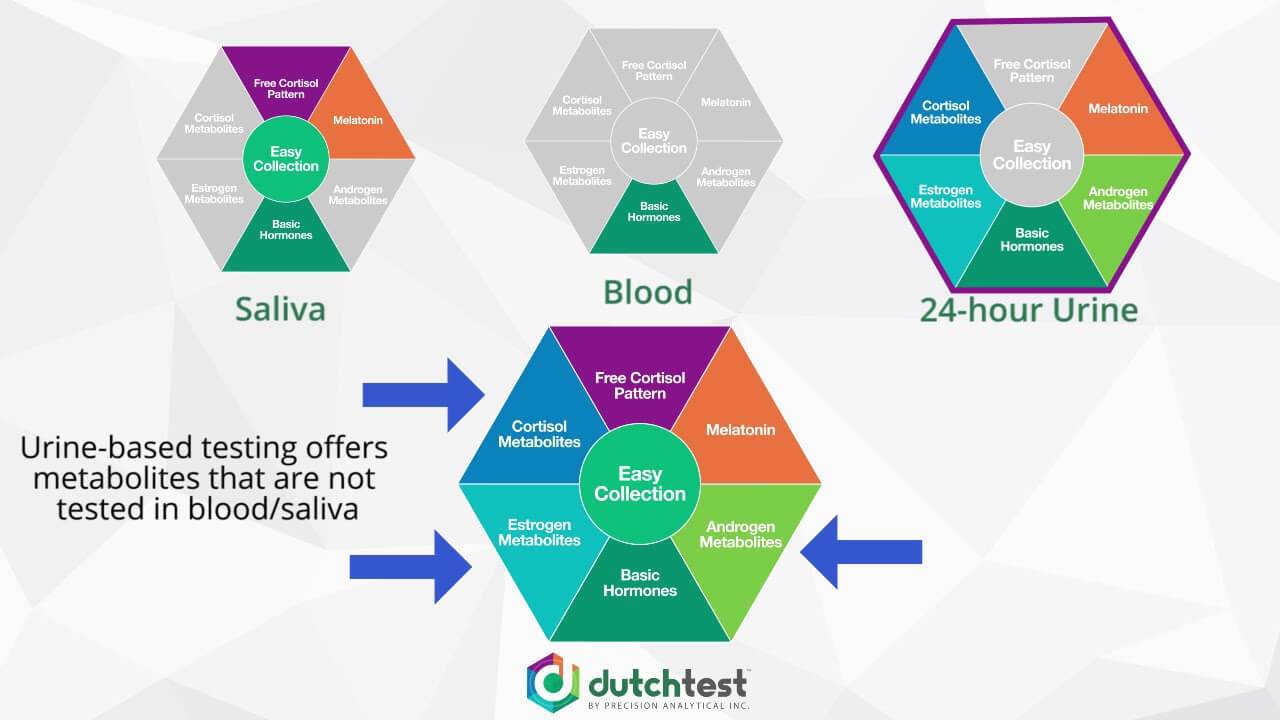
Compared to saliva tests, DUTCH measures the metabolites of the sex hormones androgen and estrogens. Blood serum tests cannot test the stress hormone, cortisol, throughout the day. The last way to test hormones is also a urine test, but this way involves carrying around an empty container that the patient must pee into throughout the day. This can be challenging for a variety of reasons.
The DUTCH involves 5 small strips that the patient urinates on during different times of the day and then the strips are allowed to dry. This test is relatively easy to perform and it covers a comprehensive range of biomarkers and results. The compliance is very good for the DUTCH and the results give a lot of feedback data for hormonal analysis.
It is wise to consider this test if you are experiencing depression, fatigue, facial hair, thinning hair, breast cancer, fibrocystic breasts, decreased libido, uterine fibroids, hot flashes, weight gain, anxiety, PCOS, infertility and endometriosis.
As a clinician, most of the DUTCH tests that I run are with women, but men also benefit from getting their hormones properly tested. Like the symptoms above, if men experience, muscle loss, gynecomastia (man boobs), loss of mental drive, low libido, depression, anxiety, prostate issues and infertility issues should consider this test.
Stress and Your Hormones:
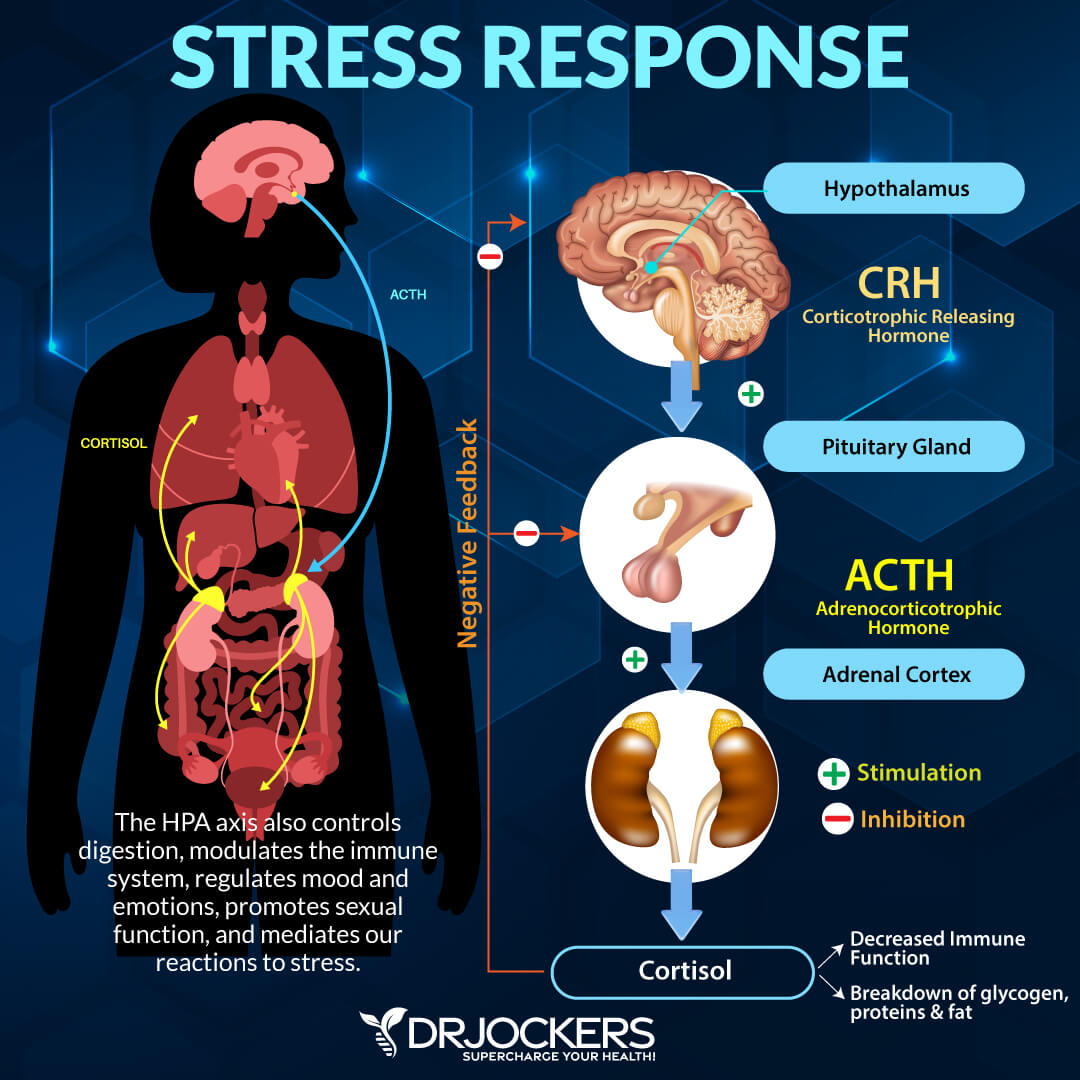
A portion of the brain called the hippocampus is what senses danger and sends signals triggering the H-P-A Axis. The Hypothalamus (H in the HPA) is a small part of the brain that sends a hormone called the Corticotrophin Releasing Hormone (CRH) which activates the powerhouse gland called the Pituitary (P in the HPA.)
The pituitary gland is the master hormone producing gland of the body. The pituitary gets stress signals from the hypothalamus and sends a hormone called Adrenocorticotropic Hormone (ACTH.) ACTH then signals the adrenal glands. Once the adrenal glands receive the message it releases cortisol, epinephrine and norepinephrine into the body.
This is a normal, natural response of the body and does not cause any problems. This is unless your body is always sensing a stressful response. When you have a chronic stress response it leads to something called cortisol resistance where the body either underproduces cortisol, clears it too fast or downregulates cortisol receptors. This condition often causes fatigue and mental lethargy and is commonly referred to as “adrenal fatigue.” (1)
Cortisol resistance causes a problem because cortisol provides a negative feedback to the pituitary and hypothalamus glands. This means the body is telling the brain that it received the message and if the stressor has stopped then the HPA axis reduces its activity and the body resets its balance and homeostasis.
However, if there is still a “perceived” threat, then the HPA axis remains highly activated while cortisol, epinephrine and norepinephrine are continually released into the body. Cortisol, epinephrine and norepinephrine are called glucocorticoids in that they come from the adrenal cortex and their main responsibility is to increase blood glucose to prepare the body for fight or flight.
When glucocorticoids are out of balance (either too high or low) for an extended period some functions of the body do not get prioritized. Such functions are some aspects of the immune system, digestion, kidney function, reproduction functions, growth, collagen formation, protein synthesis and bone formation (2).
HPG Axis
There is a lesser-known axis that we need to talk about because it crosses over with the HPA axis. The primary role of the HPG axis is control reproduction but is also important for the puberty and development as well as the immune system. Since the HPG axis is integral for reproduction, it is essential we talk about it when dealing with DUTCH tests.
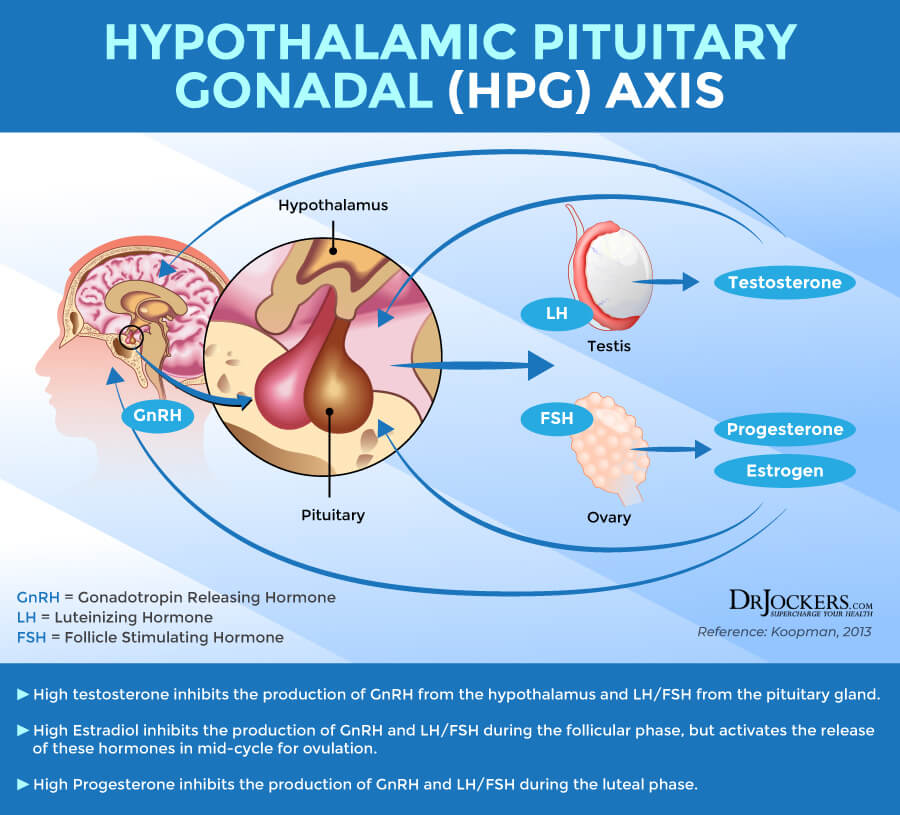
The hypothalamus also starts the HPG axis and releases Gonadotropin-Releasing Hormone (GnRH.) This signals the Pituitary to release 2 very important hormones, Luteinizing Hormone (LH) and Follicle Stimulating Hormone (FSH.) LH and FSH signal the Gonads to produce estrogens, progesterone, and testosterone.
Like the HPA Axis, cortisol sends a negative feedback signal to the pituitary gland and hypothalamus. As long as the perceived stressor is removed, it turns off the HPA Axis. Estrogens and progesterone also signal the hypothalamus and pituitary glands. Estrogens provides positive feedback in that it keeps the HPG Axis going, while progesterone provides negative feedback to deactivate the HPG Axis.
During the menstrual cycle, estrogens prepare the follicle in the ovaries and the uterus for ovulation and implantation. When the egg is released, progesterone blocks the hypothalamus and pituitary from releasing LH and FSH. If the egg is fertilized, the fetus takes control of the progesterone production. If there is no fertilization, progesterone than declines, which allows the LH and FSH to be released. This then continues the process month after month.
Chronic stress inhibits the HPG Axis at every instance, at the hypothalamus, pituitary and the gonads. It reduces production of GnRh in the hypothalamus, reduces production of FSH and LH in the pituitary, and it reduces secretion of estrogens, testosterone and progesterone out of the gonads (3, 4).
Cortisol:
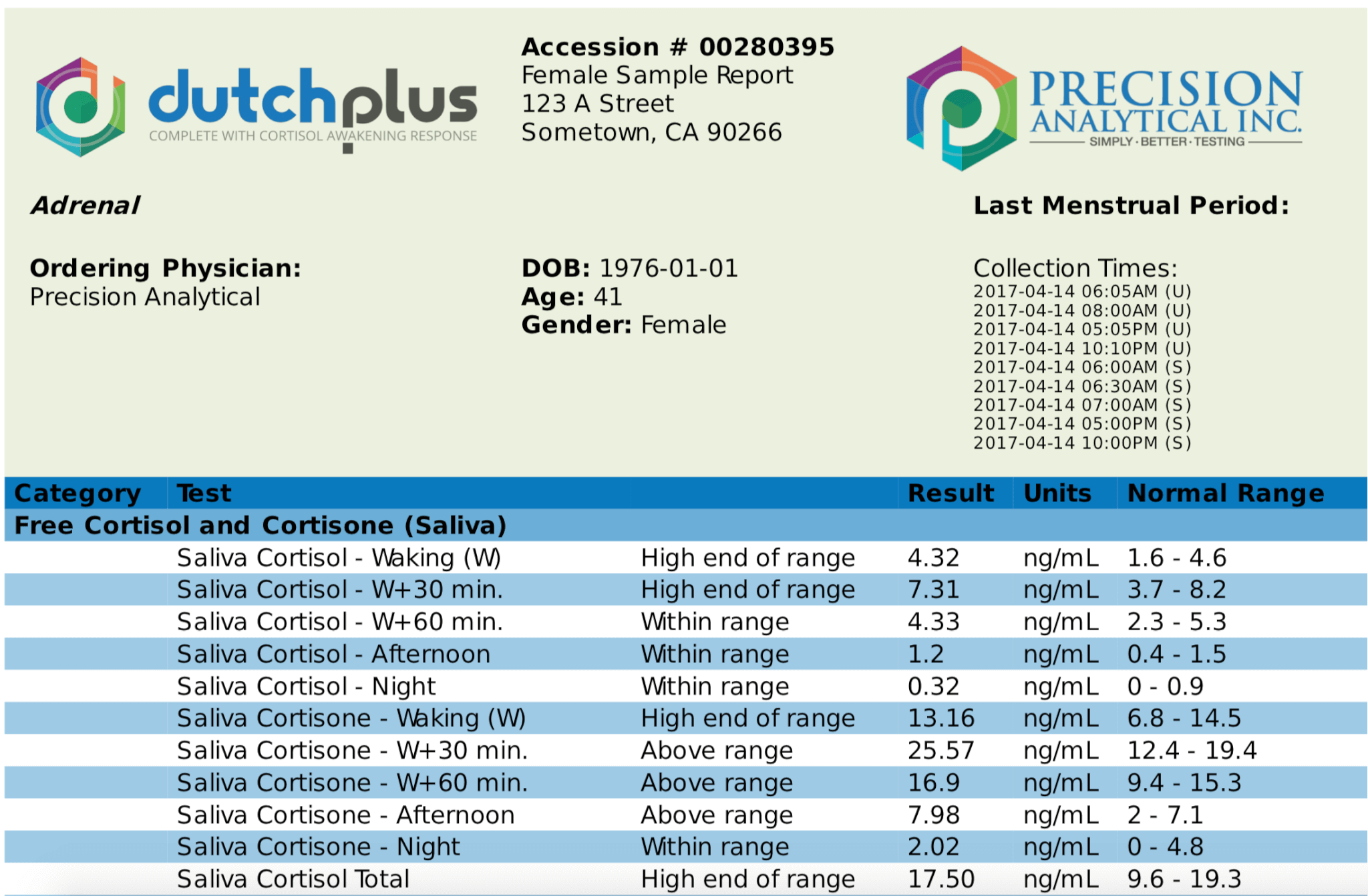
Cortisol is a hormone which is produced in the cortex of the adrenal glands. The fact that DUTCH test looks at free cortisol throughout the day is what allows it to stand out from other hormone tests.
In saliva tests, for example, the patient must take samples at very specific times throughout the day. This only becomes reliable if the patient’s normal circadian rhythm (wake and rest cycle) is when test samples need to be taken. With DUTCH samples, they are taken upon waking (whenever that may be), 2 hours after being awake, dinner time and lastly, bedtime.
Cortisol has a bad reputation because it is typically released in response to stress. A response to stress is a good thing. If we look back at our ancestors that were hunters and gatherers, responding to stress helped with reactions and alertness. If a sabretooth tiger attacked them, they were thankful for their fight or flight stress response.
Where cortisol becomes detrimental is when someone is in a constant perceived fight or flight response. The important word here is perceived. So many people today are in a constant state of fear and angst toward an imaginary stressor.
Importance of Free and Total Cortisol
It is important to measure the amount of free cortisol as well as total cortisol produced in order to get a full view of cortisol production and use in the body. The amount of total cortisol produced and the amount of free cortisol available can be very different in some scenarios. The DUTCH test really helps understand the cortisol metabolism scenario.
Our body uses various proteins such as albumin to bind to hormones in the body. Free cortisol is the cortisol found not attached to any proteins. This is the active form of cortisol and only about 1% of all cortisol is free from any substance. If someone has low free cortisol, it means just that, the amount of free cortisol in the system is low and is independent of the total cortisol produced.

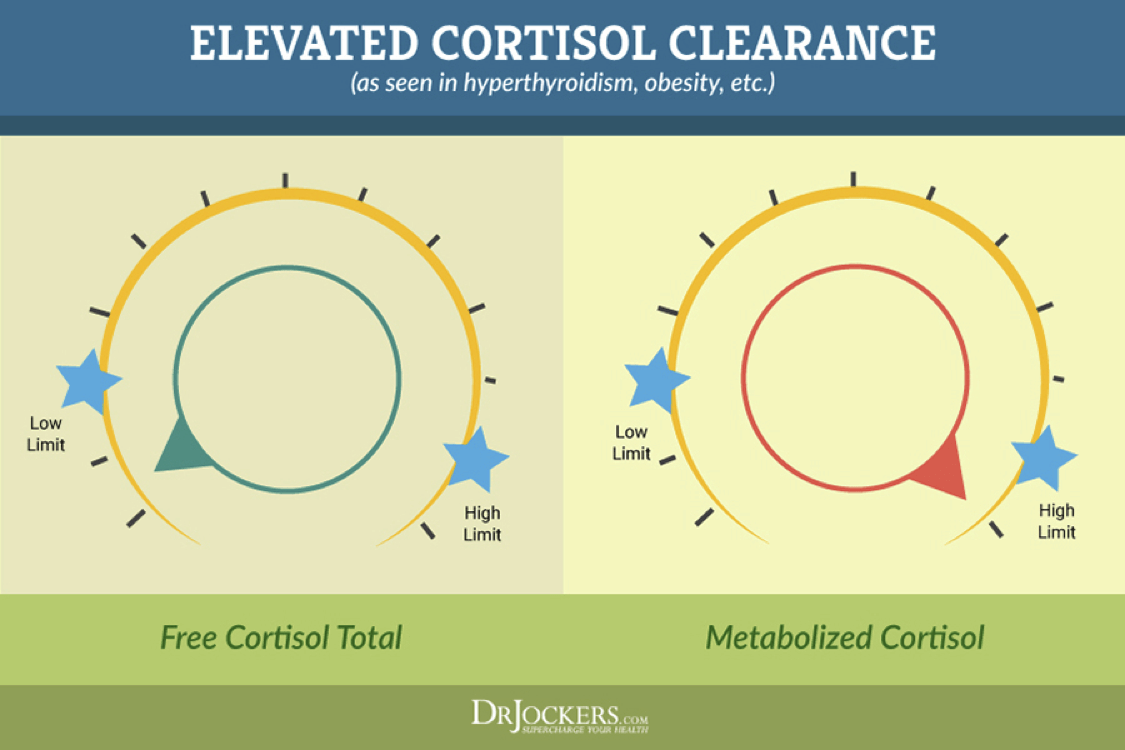
Another measurement that is important is the amount of metabolized cortisol. Our body breaks down cortisol in the liver to 3 main metabolites, a-tetrahydrocortisol (aTHF), b-tetrahydrocortisol (bTHF), and b-tetrahydrocortisone (bTHE). Metabolized cortisol is the sum of these cortisol metabolites.
Measuring both the free cortisol as well as the metabolized cortisol allows for insight into the rate of cortisol clearance/metabolism. For example, higher levels of metabolized cortisol (compared to free cortisol) are often seen in obesity where visceral fat is likely pulling cortisol from its binding protein and allowing for metabolism and clearance.
The adrenal gland has to keep up with this cortisol sequestering and excretion, so cortisol production is often quite high (as seen in the levels of metabolized cortisol) even though free cortisol does not correlate positively with adipose tissue or BMI. This insight is quite helpful for those looking to lose belly fat and suspect cortisol/stress is a major factor.
These patients are often misdiagnosed as having low cortisol production when only free cortisol is measured. Increased cortisol clearance may also be seen in insulin resistance, hyperthyroidism, chronic stress, long-term corticosteroid usage and is suspected to be part of the chronic fatigue story as well.
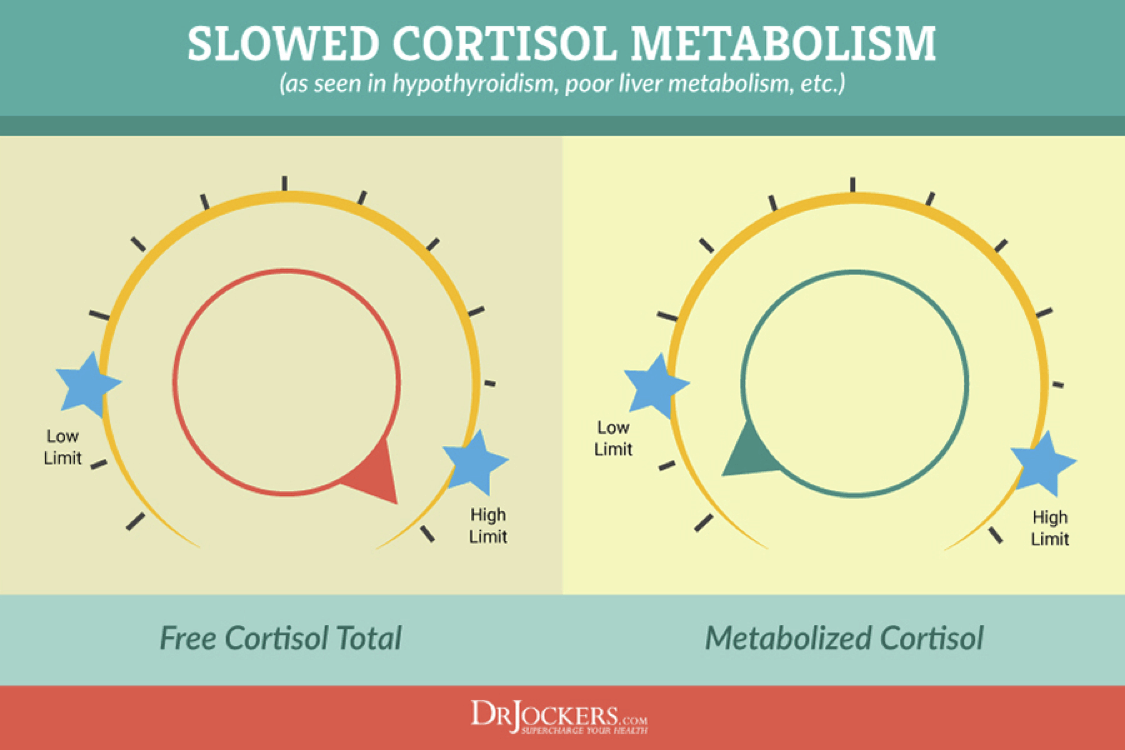
Hypothyroid or Sluggish Liver Pattern
In patients with low thyroid, the opposite pattern is often seen. When the thyroid slows down or if there is peripheral hypothyroidism where free T3 cannot get into the cells, the clearance (or metabolism) of cortisol through the liver slows down.
As a result, free cortisol starts to increase and may show up elevated on the DUTCH Test. The literature is more definitive for lower metabolized vs. higher free cortisol, but these are commonly seen together. The liver is responsible for metabolizing cortisol, so this pattern is also indicative of sluggish liver metabolism.
To summarize, if free cortisol is high and metabolized cortisol is low, you have to think sluggish liver function and possibly low thyroid hormone. You can confirm with blood testing for thyroid hormone, especially free T3 levels and looking at estrogen metabolism for signs of sluggish liver function.
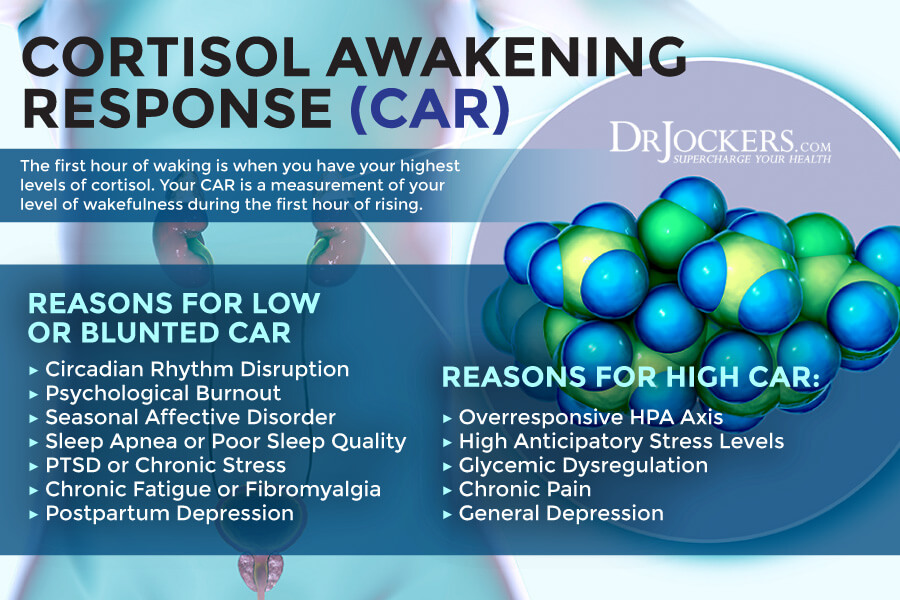
Cortisol Awakening Response
Cortisol is responsible for waking us up in the morning and giving us a level of wakefulness as we get out of our bed and begin our day. We call this the Cortisol Awakening Response or CAR. When your HPA axis is disrupted, it can lead to either an overproduction or underproduction of cortisol upon rising.
When we open our eyes upon waking, cortisol levels naturally begin to rise by an average of 50%. 30 minutes after waking, cortisol levels will still show this sharp increase. By 60 minutes after waking, cortisol levels have peaked and begin to decline. The DUTCH test measures some of the parameters of this test so you can assess the CAR.
If this doesn’t happen properly it can lead to fatigue, brain fog and daytime sleepiness and in some cases, insomnia at night. Many people have trouble getting out of bed in the morning or they need a lot of caffeine to get their brain working right. These are both classic signs of a sluggish cortisol awakening response.

This can be a result of an underactive HPA axis, excessive psychological burnout, seasonal affective disorder (SAD), sleep apnea or poor sleep in general, PTSD, chronic fatigue and/or chronic pain. A decreased CAR has also been associated with systemic hypertension, functional GI diseases, postpartum depression, and autoimmune diseases (5, 6, 7).
Other people have high morning blood sugar levels and may experience anxiety, heart racing or mid-morning or mid-day fatigue which are all signs that the cortisol awakening response was too high and therefore when the cortisol levels taper off, they often drop too low and cause fatigue later in the morning or mid-day.
This can be a result of an over-reactive HPA axis, ongoing job-related stress (anticipatory stress for the day), glycemic dysregulation, pain (i.e. waking with painful joints or a migraine), and general depression (not SAD).
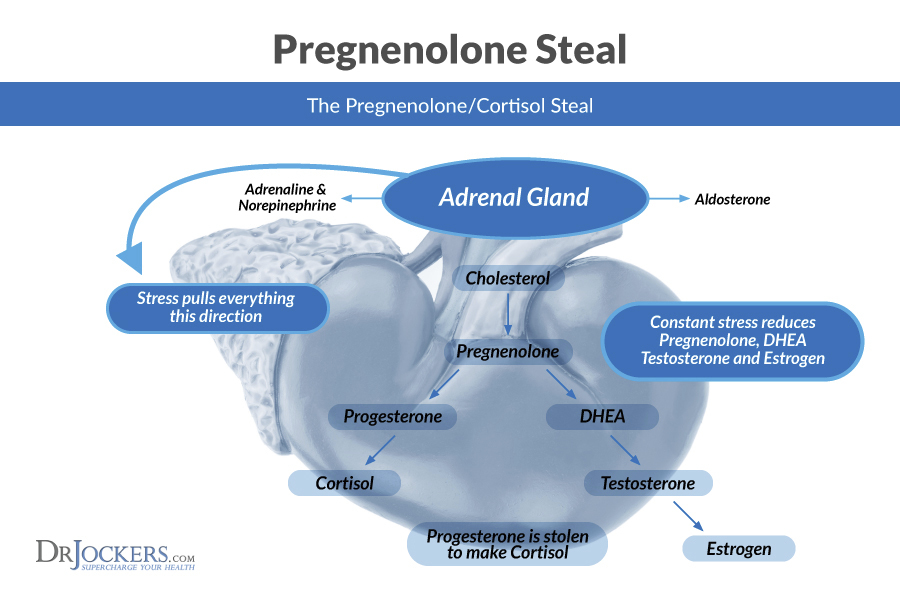
Pregnenolone
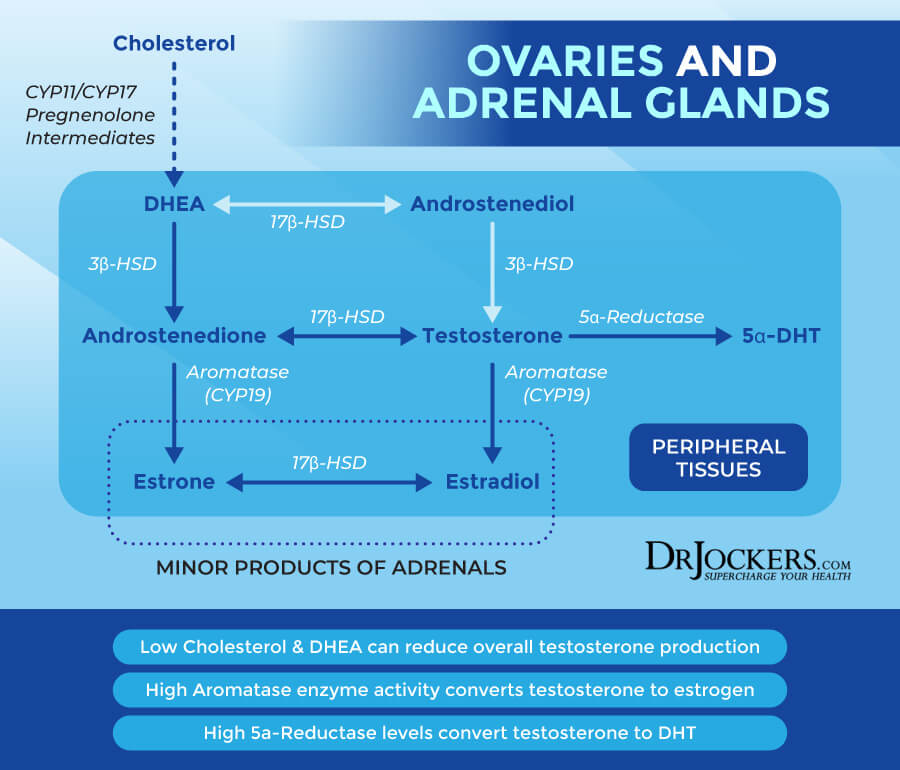
Pregnenolone is often called the “mother hormone” and is produced in the body by cholesterol. Yes cholesterol. Cholesterol is at the very core of all of our hormones. Cholesterol makes pregnenolone and then is the precursor to progesterone, DHEA, which then leads to the synthesis of testosterone and the estrogens.
Pregnenolone is produced in the astrocytes and oligodendrocytes, which are specialized cells found in the central nervous system. The oligodendrocytes also produce the myelin sheath, which is the fatty insulation which surrounds all of our nerves. Pregnenolone has been scientifically shown to aid in depression, anxiety, schizophrenia, Alzheimer’s disease and many more.
When there is an increased demand for progesterone, there has to be an increase in pregnenolone. Since pregnenolone is the precursor to so many different hormones in the body, and more is being used to create progesterone and thus cortisol, this is called “pregnenolone steal” in the body because it is taking the raw materials away from making our important sex hormones (8).
The Role of Pregnenolone in Building Hormones
In other testing, the test may just be testing estrogens or testosterone. If it is found to be low, the general approach is to do hormone replacement therapy (HRT.) Where the patient is given either estrogens or testosterone, depending on what was found to be low on the tests. Hopefully you are seeing why this can be a very dangerous approach.
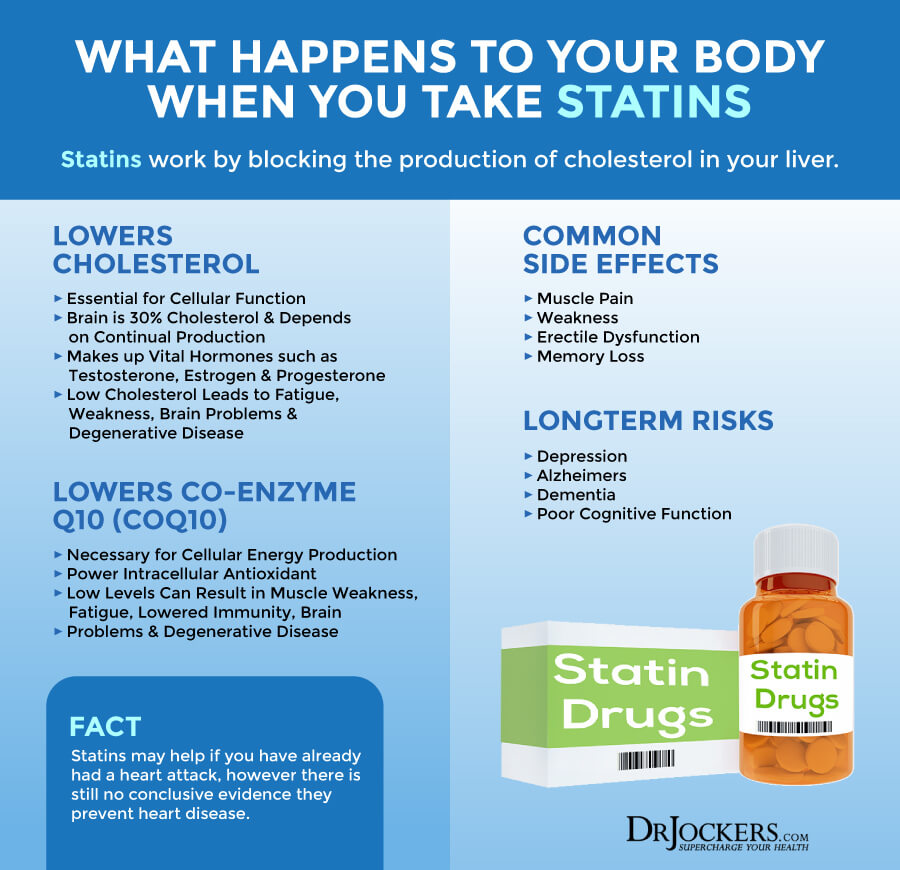
If there has been no “upstream” testing, you actually have no idea if there is a deficiency somewhere else. What if you are taking cholesterol lowering medications?
Your body is demanding more raw material because it is chronically stressed so it is increasing your body’s natural process to create cholesterol, to then increase pregnenolone, to increase progesterone, to then create more cortisol. If the stressful environment still exists and the patient is trying to get pregnant, has menstrual issues, low testosterone symptoms, there has to be an increase in cholesterol to make all of our hormones.
Cholesterol has been unfairly vilified, in my opinion. Because of this, there has been a lot of unnecessary HRT drugs used by patients. Especially in conjunction with cholesterol lowering medication. There actually might not be an issue with testosterone or estrogen production. The issue could be something as far upstream as not having enough cholesterol in the system.
Pregnenolone Deficiency
A deficiency of pregnenolone can lead to such symptoms as decreased sex drive, depression, fatigue, impaired memory, loss of bone density and decreased muscle mass. Also, because it is considered the “mother hormone” if it is decreased, then there will be decreased in all other hormones.
Clinically, I see patients with PCOS (Poly Cystic Ovarian Syndrome), high insulin, hyperglycemia, stress and elevated alcohol use can lead to lower levels of pregnenolone on the DUTCH test. There can be elevated pregnenolone and that is found in a genetic disorder called Congenital Adrenal Hyperplasia (CAH.) This causes a deficiency in enzymes required to convert pregnenolone to its different sex hormones.

Progesterone:
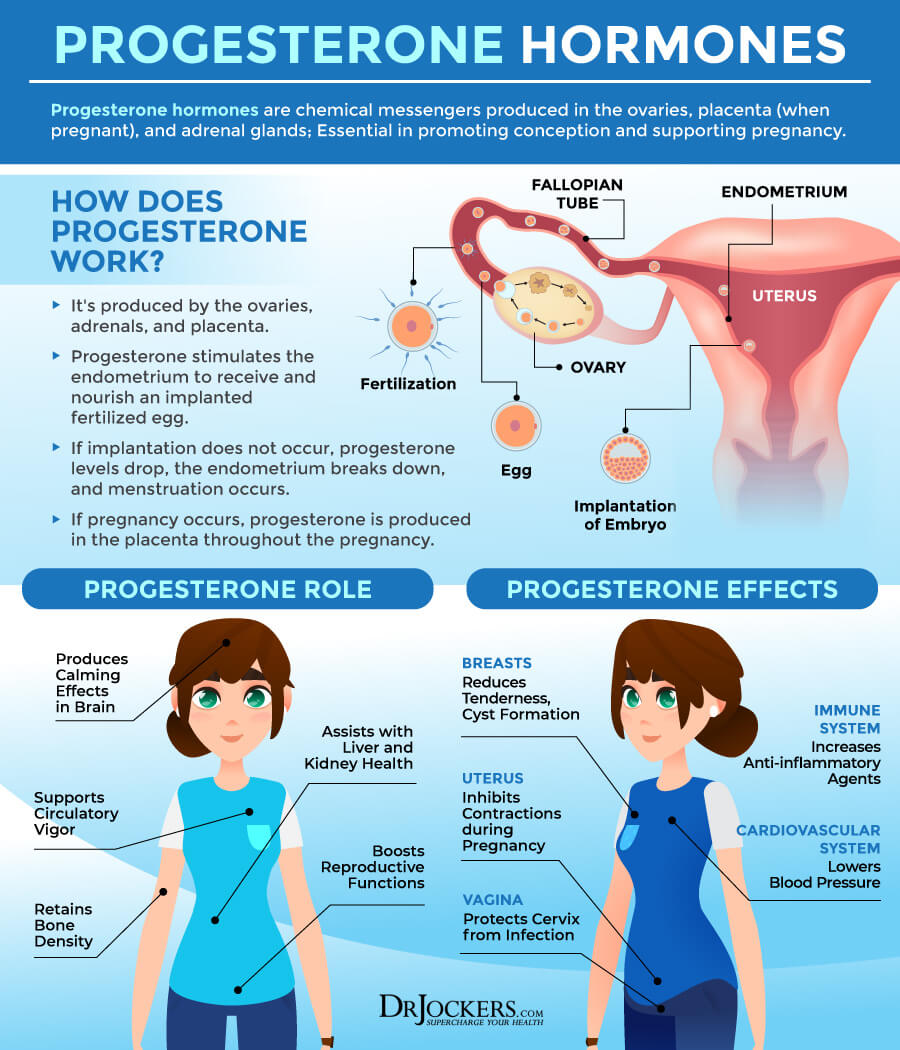
Progesterone is found in both men and women, but it clearly has a different role in each. In women, as stated above in the HPG axis, progesterone gets the body ready for potential pregnancy. Progesterone levels rise in the second half of the menstrual cycle and following the release of the egg, or ovulation.
This why it is ideal to perform your DUTCH test between days 19–22 of a standard 28-day cycle. Progesterone is mainly produced by the corpus luteum and gets the endometrium ready to receive an implanted fertilized egg. If implantation does not occur, estrogen and progesterone levels drop, the endometrium breaks down and menstruation happens.
If pregnancy does occur, progesterone is produced by the placenta, and levels remain elevated throughout the pregnancy. The combination of high estrogens and progesterone throughout the pregnancy suppresses further ovulation. Progesterone also leads to milk-producing glands to develop during the pregnancy.
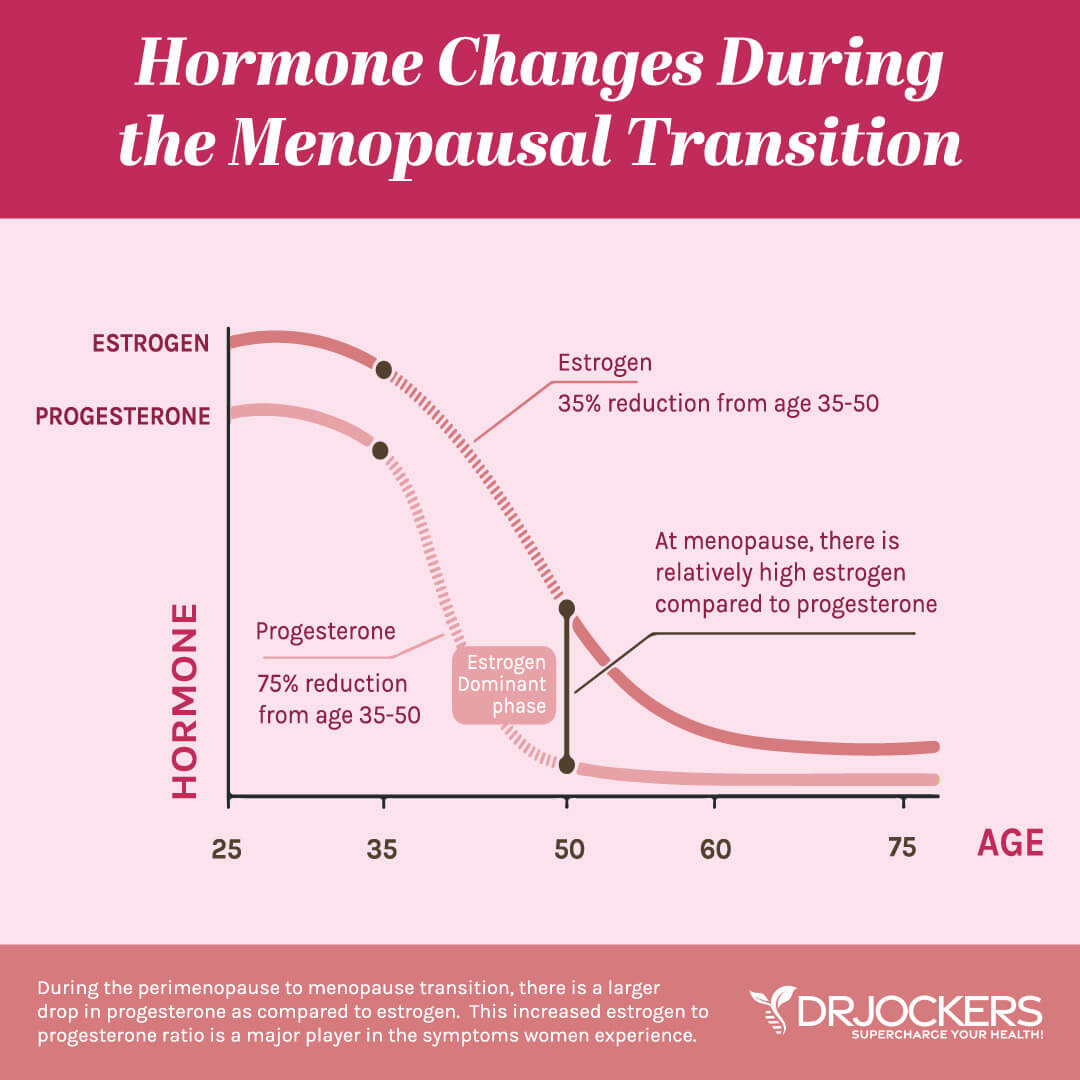
Estrogen to Progesterone Ratio
Progesterone is a key player in women’s hormones because it is typically looked at as an Estrogen:Progesterone ratio. A woman can be estrogen dominant if she has too many estrogens but can also be due to low progesterone. Yet another reason why just taking HRT is not always the best approach and why a lot of women do not notice any difference if they start taking these dangerous drugs.
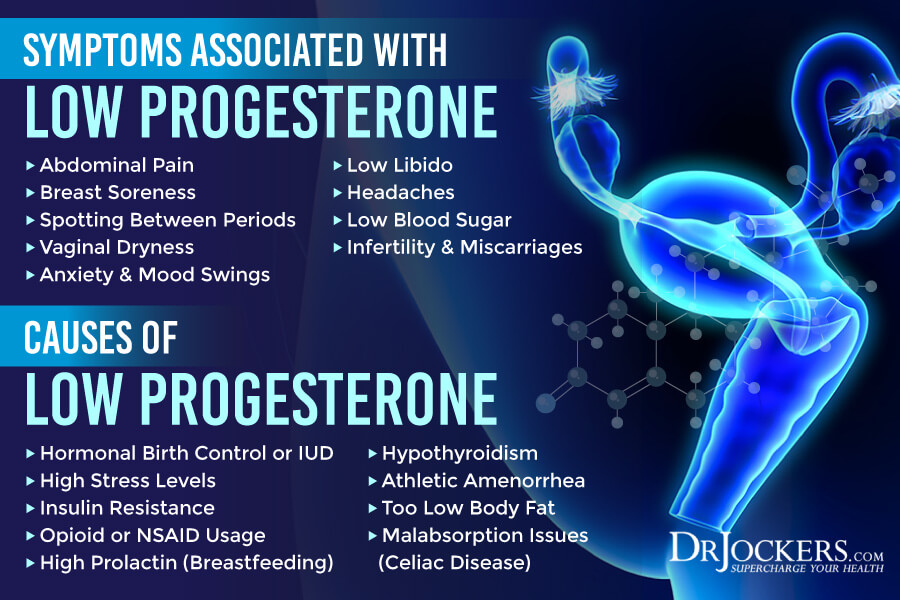
When high progesterone is found on a lab, this usually is an indicator that the patient is pregnant or can be the result of the patient being on a pregnenolone or progesterone supplement. Decreased progesterone is seen in the following: (9)
Hormonal Birth Control or Hormonal IUD
Under High Stress
High Insulin
Opioid or NSAID Use
High Prolactin (due to milk producing glands being made)
Hypothyroidism
Being Underweight
Women with low progesterone can notice symptoms such as, abdominal pain, sore breasts, spotting between periods, vaginal dryness, depression, anxiety and mood swings. They can also notice low libido, low blood sugar, headaches or migraines. It is normally difficult for women with low progesterone to get pregnant, but if they do, they have a higher rate of miscarriages.
In men, progesterone is produced in the testes as well as a small amount in the adrenal glands. Even though men do not have menstrual cycles, progesterone is still necessary, just not in as high amounts as women. This is because progesterone is a precursor to testosterone.
Men with low progesterone levels will also experience low testosterone. Low progesterone can lead to depression, irritability, low libido, erectile dysfunction, muscle loss, fatigue and memory loss (10). The DUTCH looks at progesterone metabolism in great detail.
High progesterone levels are not a good thing either. This can also be caused by PCOS, ovarian cancer, and adrenal gland disorders. These symptoms are very similar to PMS symptoms, such as breast swelling, breast tenderness, bloating, anxiety, agitation, fatigue, depression, low libido, and weight gain.
Testing Progesterone Levels:
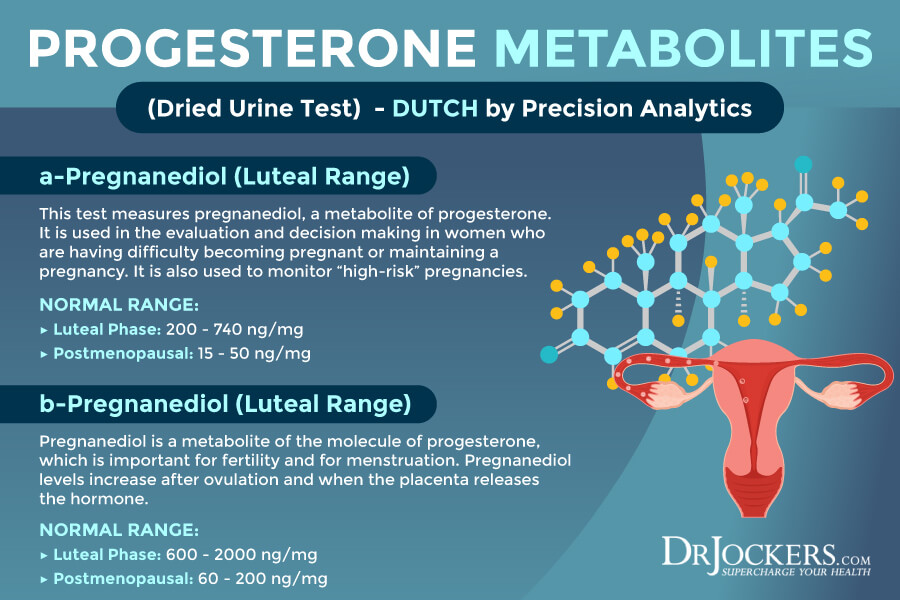
The way that progesterone is measured is through its metabolites a-Pregnanediol and b-Pregnanediol. These pregnanediol forms are the most easily measured metabolites of progesterone. Measuring them both together gives the full understanding of what is happening with progesterone production and metabolism.
The luteal phase is when there is the largest rise in progesterone, so the levels are higher. The normal ranges here are 200–740pg for a-Pregnanediol and 600–2000pg for b-Pregnanediol. The DUTCH test also has a range if the samples were taken during the follicular and ovulatory phases which are 25-100pg for a-Pregnanediol and 100-300pg for b-Pregnanediol. Finally, menopausal women have the lowest production and their ranges are 15–50pg for a-Pregnanediol and 60–200pg for b-Pregnanediol.
The reason why it is important to test both the alpha and beta pathways is due to the unique biochemistry patterns of each individual. One woman may move progesterone more down the alpha than the beta pathway and vice versa. Testing both pathways ensures you are getting the most accurate measurements.
Women with PCOS tend to push progesterone down the alpha pathway and women with hypothyroidism tend to push more heavily down the beta pathway. Reporting both major progesterone pathways is just another way that the DUTCH test aims to provide the most accurate hormonal representation possible for you and your patients.
High progesterone metabolites can occur with progesterone or pregnenolone supplementation. High progesterone is also seen in PCOS when ovulation occurs because of excessive luteinizing hormone secretion (11).
Some women may naturally make high levels of progesterone and, if symptom free, it is usually not concerning. Symptoms of high progesterone may include bloating, fatigue and food cravings, especially high carb and high calorie foods.
DHEA:
Pregnenolone is a precursor to progesterone but then it can also lead to the production of DHEA. Dehydroepiandrosterone or DHEA is a hormone also produced in the adrenal glands and small amounts in the testes and ovaries, and it can produce androstenedione. This means that DHEA can lead to production of testosterone and estrogens.
There are a lot of people who use DHEA as an anti-aging therapy, work as a performance enhancer, depression therapy for menopause. Low levels of DHEA can be indicated by Addison’s disease, hypopituitarism, dementia, trouble maintaining or achieving an erection, vaginal atrophy, low sex drive, osteoporosis, AIDS, Lupus, chronic fatigue and Crohn’s disease.
High levels can be caused by adrenal cancers, PCOS as well as CAH. Symptoms of high DHEA can be acne, deep voice, hair loss, irregular periods, sterility.
This might seem like a recurring theme of this article, but you should not just take a supplement because you might be experiencing a symptom stated. It should also be incredibly clear if you are having hormonal issues, the remedy should not be to take more of that hormone.
Doing this can cause your body to down regulate the natural production of that hormone. Finding out if there is a breakdown somewhere in the pathway should be the primary focus, to then start fixing and rebuilding the pathway that has broken down.

Testosterone:
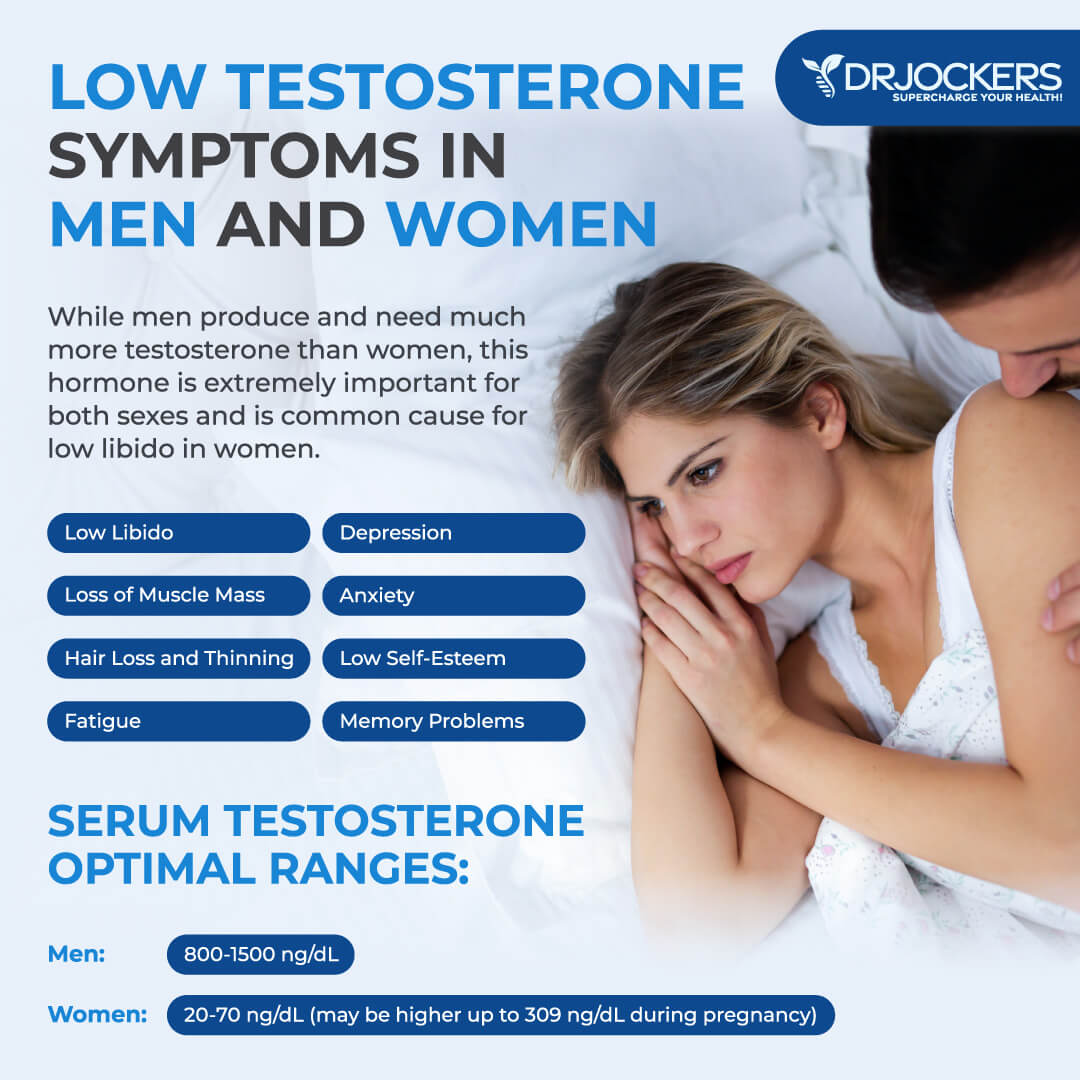
Up to this point I have discussed hormones that primarily affect women, and the DUTCH test also looks at testosterone metabolism. Testosterone gets all its notoriety on its effect on men, but women need it too.
But before we talk about testosterone we must touch on its predecessor, androstenedione. Cholesterol metabolizes into pregnenolone which then gets metabolized into progesterone.
Progesterone can then either create cortisol or become androstenedione. Androstenedione is produced in either the ovaries of women, testes of men or in the adrenal glands.
It is an androgen hormone that can be converted into testosterone or further converted from testosterone to the estrogens. Androstenedione is not a very potent hormone, but if it is elevated it can mean there is an adrenal tumor, or PCOS and can lead to excess body hair or abnormal periods.
Androstenedione is metabolized in the testes of males and ovaries of females and once again in very small quantities in the adrenal glands. When you think about what makes a man a man, people normally think Testosterone.
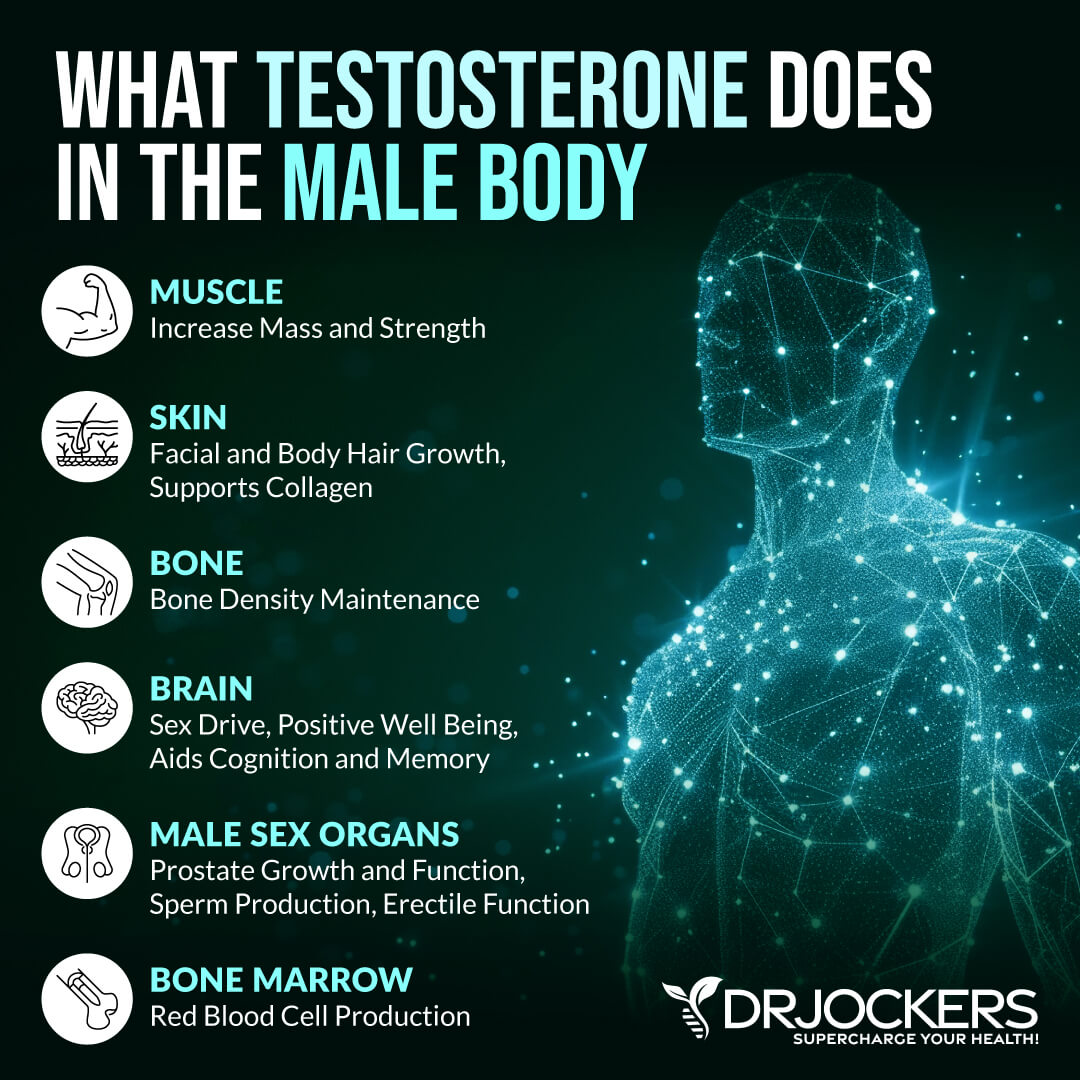
This is because it is produced in much greater levels in men. Testosterone initiates the development of the internal and external male sex organs and is essential for sperm production later on in life.
Testosterone is linked to many different changes seen in boys during puberty, increase in height, body and pubic hair growth, enlargement of the penis, testes and prostate gland, and changes in sexual and aggressive behaviors. It also regulates the secretion of LH and FSH.
In women, testosterone is produced in the ovaries and the adrenals and then gets converted to estradiol. When in a normal range, testosterone helps regulate mood, sex drive, healthy body weight. As women age, testosterone helps regulate healthy bone growth and strength and helps with cognitive health.
High Testosterone and PCOS
If women have too much testosterone, this is usually a sign of PCOS. Women suffering from this can see increased acne, body and facial hair, balding at the front of their hairline, increased muscle development and a deepening of their voice.
High testosterone interferes with monthly periods and the body’s ability to ovulate. PCOS can not only cause very uncomfortable monthly periods, and it can also cause infertility and miscarriages.
There is a lot of research on the internet that suggests PCOS can cause such health conditions as insulin resistance, diabetes, high cholesterol, high blood pressure and heart disease. I disagree. As we have seen that Cholesterol is at the root of our sex hormone pathway, then there can be a breakdown somewhere in this pathway.
I have worked with a lot of women suffering from PCOS and they have been given the common Type 2 Diabetes drug “Metformin” because there is a correlation to elevated blood sugar. I have also found that, if we help them with their diet, find the root of their inflammation, give them strategies to cope with stress, it is amazing how their blood sugar normalizes as does their PCOS symptoms.

Low Testosterone Levels
There is also a common misnomer in certain health circles that testosterone production begins to decrease after the again of 30. Once again, I disagree. I do not believe that production drops, I believe production has been on the rise and then levels out from 30 years of age until the day you die.
We have been sold a bad bill of goods so that we feel we are victims, and our only remedy is to take testosterone. Low testosterone can such symptoms as fatigue and an increased risk for bone loss, osteoporosis, and fractures.
In both men and women, testosterone is a hormone to help with “Drive” not just sex drive but to help with motivation and drive to accomplish tasks. This can be caused by obesity, opioid use, hormonal birth control, acute illness, and steroid use.
Our bodies are amazing and incredibly smart. There are checks and balances put in place for everything. What is pretty much every man in America is taking a cholesterol lowering medication.
What is the most common age for when men start taking testosterone? 40. We are artificially lowering the raw material of cholesterol through medication so we cannot make as much testosterone that is needed. Then there are the gym goers and the athletes who take anabolic steroids.
When this happens over an extended period of time, the body senses that there is more testosterone than normal in the body, so it then down regulates the natural production of testosterone. This is the reason why testes get smaller, there is an increase in abdominal belly fate and an overall decrease in “Drive.”
When testosterone goes through its normal life cycle, an enzyme 5-alpha-reductase turns testosterone into a stronger metabolite called 5-alpha dihydrotestosterone then turns into different metabolites and recycled throughout the body.
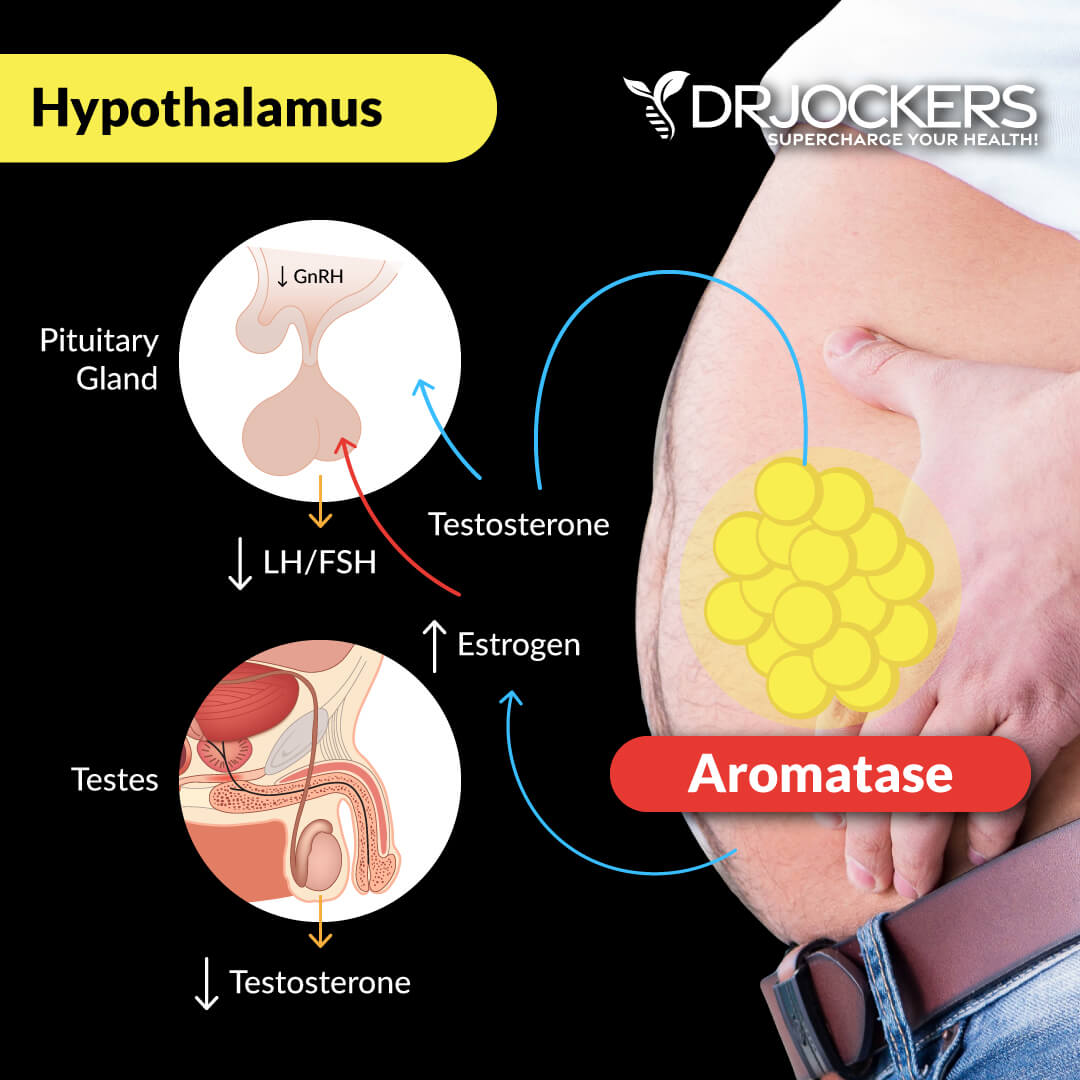
In both men and women, then testosterone is produced and needs to be turned into estrogens, it goes through a process of aromatizing. If there is an unnatural influx of testosterone, it then gets aromatized to Estradiol which keeps the testosterone and estrogen balance. When estrogens get too high, it can cause some cancers, and the drug used is an aromatase inhibitor to keep testosterone in the system.
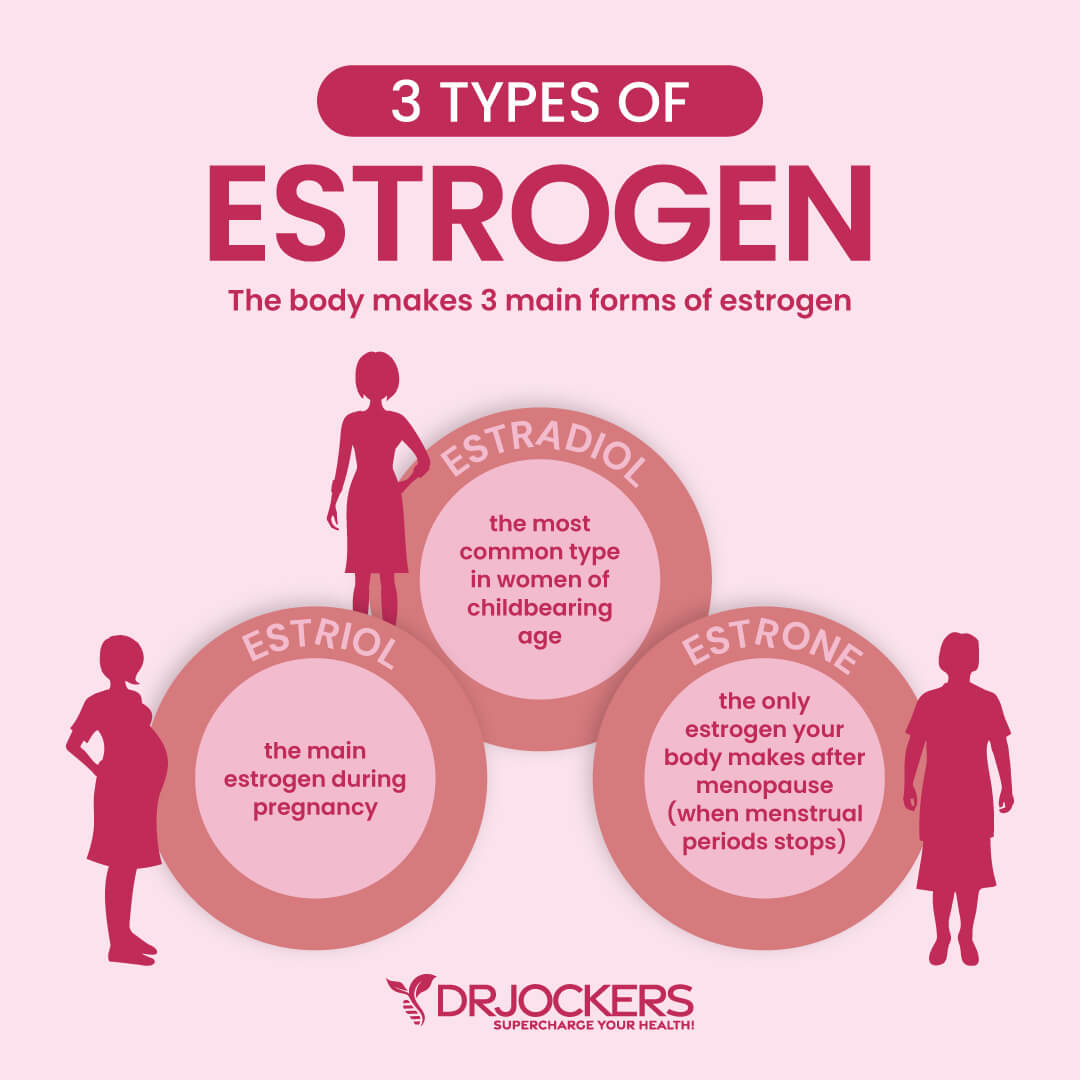
Estrogens:
Estrogen is the cumulation of Estrone (E1), Estradiol (E2) and Estriol (E3.) There is an issue with typical estrogen testing, the “estrogen” being tested can be in normal range, but you can have one or all of the estrogens outside of normal. If the “estrogen” being tested is out of normal range, it is not known which one is actually outside of normal range.
The estrogens are made primarily in the ovaries of women who still have a menstrual cycle. Small amounts can be aromatized from testosterone. If a woman is menopausal, the majority of her estrogens are produced this way. It is interesting to note that the level of estrogens is higher in men than in post-menopausal women.
The main and most potent estrogen is Estradiol (E2). It is made primarily in the ovaries and the testes but is also found it liver tissue, neural tissue and fat tissue. This is why women with really low body fat often have hormonal issues. They do not have the body fat necessary to help support estradiol production. Excessive body fat can lead to an overproduction of estradiol and estrogen dominance.
Estrone (E1) is also made in the ovaries but in fat tissue in less quantities than estradiol. Estrone is a less potent form of estrogen and is thought to be the only estrogen produced in post-menopausal women.
Although it is a less potent estrogen, high levels of estrone can still increase the risk of estrogen dominant cancers as well as estrogen dominant symptoms. These symptoms include breast tenderness, heavy menstrual cycles, fibrocystic breast changes, headaches, and erectile dysfunction and breast development in men.
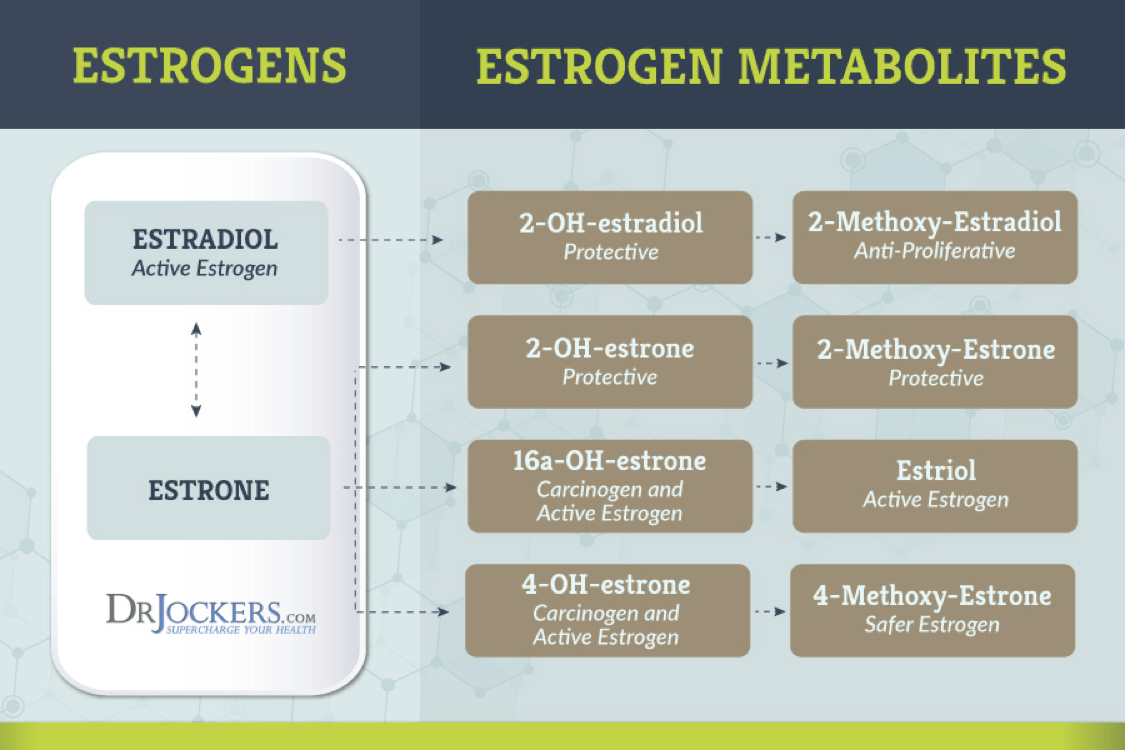
Estrogen Metabolism
Estrone is thought to be more abundant in menopause. Estradiol and estrone can interconvert into each other. Estriol (E3) is the third estrogen and is produced in significant amounts during pregnancy.
In men and women, estriol is irreversibly produced by estradiol or from estrone through 16OH-Estrone which makes it the largest circulating estrogen because both Estrone and Estradiol can make it. Despite this, Estriol is not nearly as potent as Estradiol. Estradiol is actually 80x more potent.
When reviewing the estrogens on the DUTCH, you want to take a good look at the 16a-OH estrone and the 4-OH estrone as these metabolites have very strong growth promoting signal and high levels of these metabolites are associated with higher risk of fibrocystic breast disease, endometriosis and breast, uterine and ovarian cancers.
Estrogen and Liver Metabolism
When looking at the DUTCH test results you will see the word metabolites or metabolized. When your body makes an estrogen or cortisol or if someone takes a hormone by HRT, it must be processed by the body in the liver through the process of phase 1 and 2 detoxification before it can be excreted out of the body.
This is known as hormone metabolism. As a hormone undergoes this process, it gets changed into other forms called metabolites. It might also be a coincidence that cholesterol is produced in the liver. The very beginning and the very end of hormone synthesis is in the liver.
This is important because after estrogens go through phase 1 detoxification it moves on to methylation. Methylation neutralizes the phase 1 metabolites and prepares them to be excreted out of the body instead of sending them back into circulation. If a patient has a genetic issue called MTHFR they have issue methylating and the reports tells you where you are on the methylating spectrum.
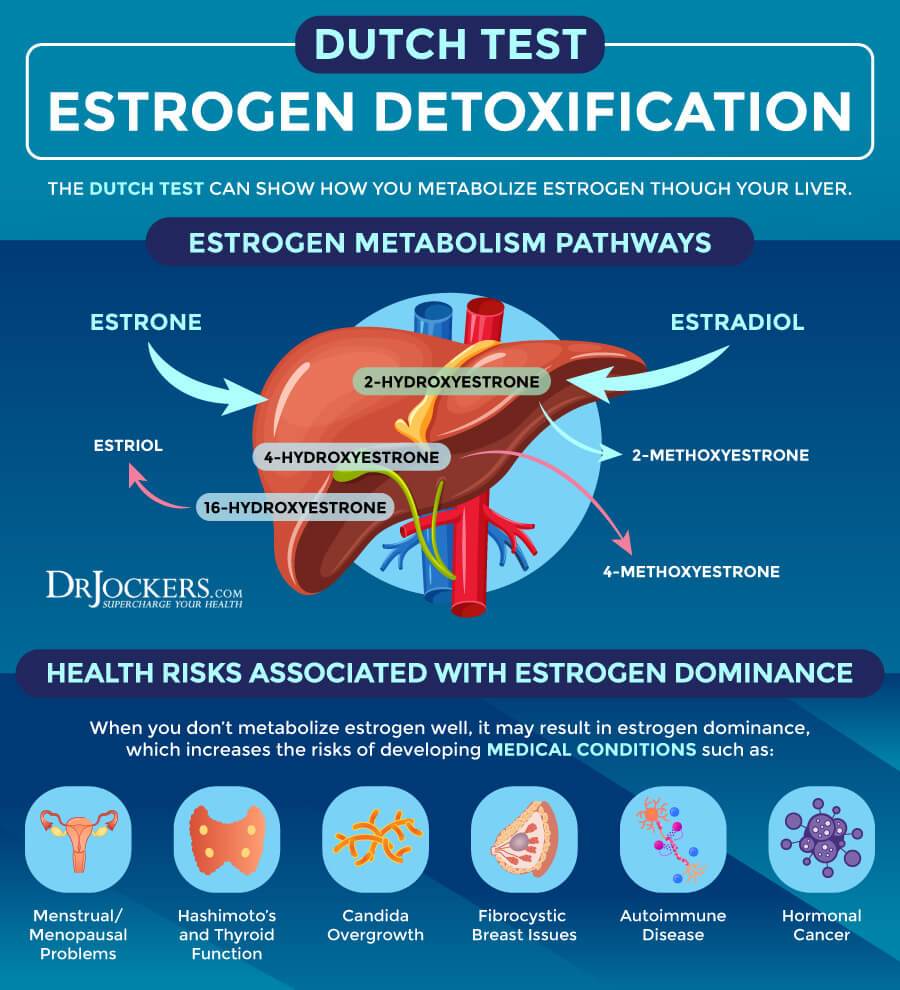
Estrogen Imbalances
Ovarian hyperproduction of estrogens, PCOS, environmental/xenoestrogen exposure, alcohol use, obesity, over aromatizing, inflammation and insulin resistance can lead to elevated estrogen levels. Symptoms of having elevated estrogens in women is mood swings, weight gain, breast tenderness, fibrocystic breasts, heavy menses, fibroid/polyp development. In men, breast development, weight gain, and mood swings happen.
Low estrogens can be caused by irregular cycles, no cycles, menopause, ovarian insufficiency, removal of ovaries (hysterectomy), hypothyroid, anorexia, hormonal birth control, head trauma affecting the hypothalamus and pituitary function. The symptoms of this happening is fatigue, depression, hot flashes, night sweats, vaginal dryness, pain with intercourse, low libido, joint pain, brain fog, migraines/headaches, fertility issues and dry skin.

Cortisone:
Cortisone is the inactive form of cortisol. Cortisol can be converted to cortisone in the kidneys, colon and salivary glands. Cortisone can also be converted back into cortisol in the liver. Here is a key reason why the DUTCH test is so accurate. What you see in the urine as free cortisone actually reflects free cortisol that enters the kidneys and is converted to cortisone locally before excreted.
This makes free cortisone a secondary, confirmatory for the up and down pattern of free cortisol. When free cortisol and free cortisone are both high, it confirms elevation. When free cortisol is high and cortisone is not, free cortisol levels may not be quite as high as the cortisol levels themselves imply.
Or it could mean free cortisol is elevated due to a metabolic preference more so than an increase in production. The relationship between free cortisol and free cortisone tells providers some information about how sharply the kidney is deactivating cortisol. But it does not tell us systemically which one is predominating.
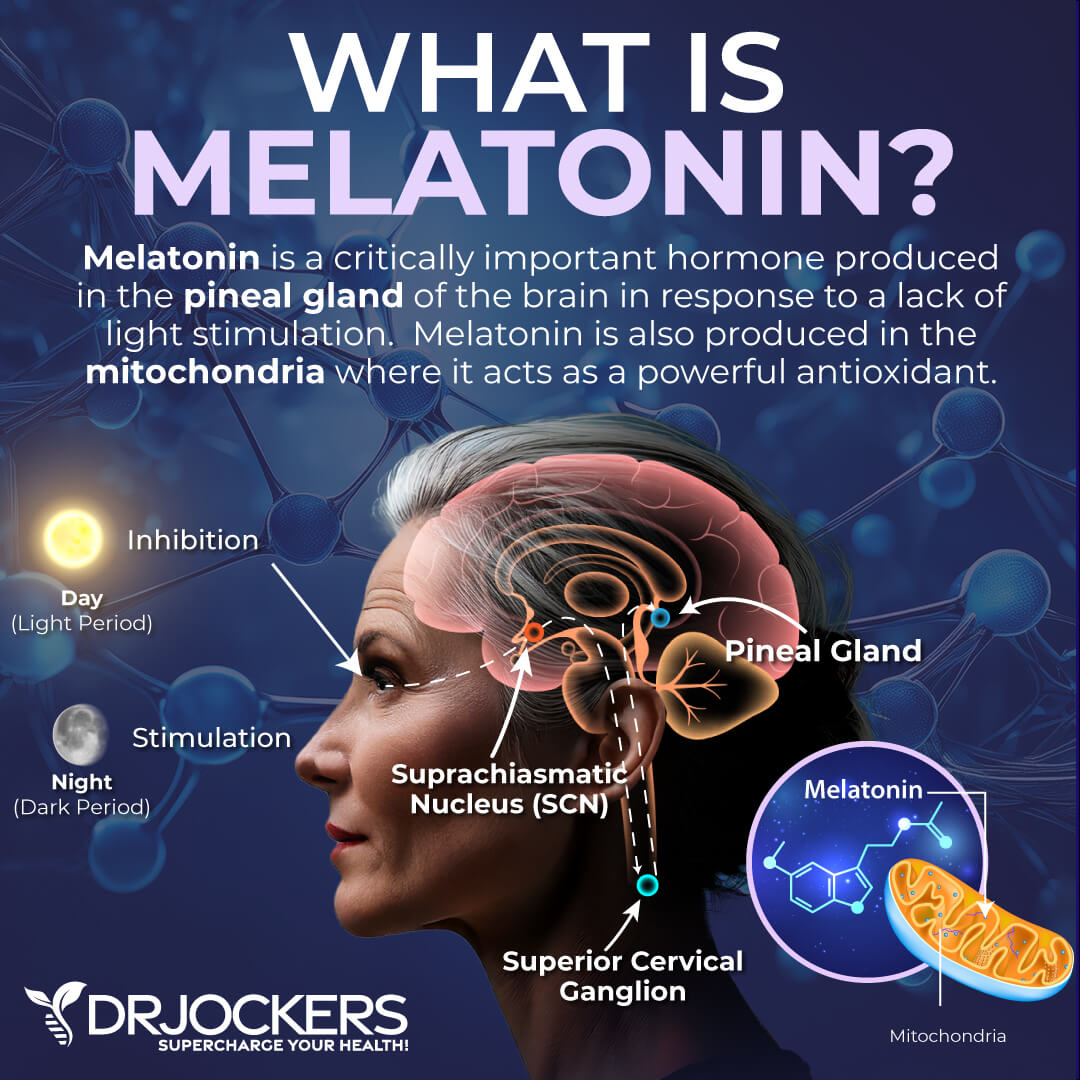
Melatonin Levels
Melatonin is a nutrient that’s important for a healthy sleep-wake cycle. It is often used as a supplement for insomnia, jetlag, and improving other sleep problems. It is also a powerful brain detoxification agent.
Melatonin helps to clean environmental toxins and other pathogens from your brain. A 2010 study published in Current Neuropharmacology has found that melatonin helps to inhibit pro-inflammatory cytokines, offers antioxidant support, and reduces inflammation, oxidative stress, and infections (12). As a result, it may be a powerful protective agent for traumatic brain injury (TBI) patients reducing inflammation and infections.
A 2019 study published in Death and Disease has also found that melatonin helps to reduce inflammation (13). A 2010 study published in Current Neuropharmacology has found that melatonin deficiency plays a role in oxidative stress and age-related neurodegeneration (14).
Another 2010 study published in Current Neuropharmacology has found that because melatonin can cross the blood-brain barrier, it can effectively fight neurotoxin agents that may also pass this barrier (15). It stimulates antioxidative enzymes, fights free radical damage, and helps to reduce neurotoxins at the mitochondrial level. As a result, melatonin not only supports your sleep but helps to protect your brain and neurological health.
The DUTCH test looks at melatonin levels upon waking in the morning in the form of 6-OH Melatonin sulfate. While this is a morning test, it is adjusted to reflect the amount you should have at night. The normal range on the DUTCH test is 10–85 ng/mg, although the optimal range we like to see is roughly 30–65 ng/mg.
Nutritional Organic Acid Markers:
The DUTCH Comprehensive test also looks at several nutritional organic acid markers that give insight on the metabolism of vitamin B6, B12 and glutathione. These nutritional markers are important for understanding the methylation and detoxification processes involved in phase II liver detoxification and cellular metabolism.
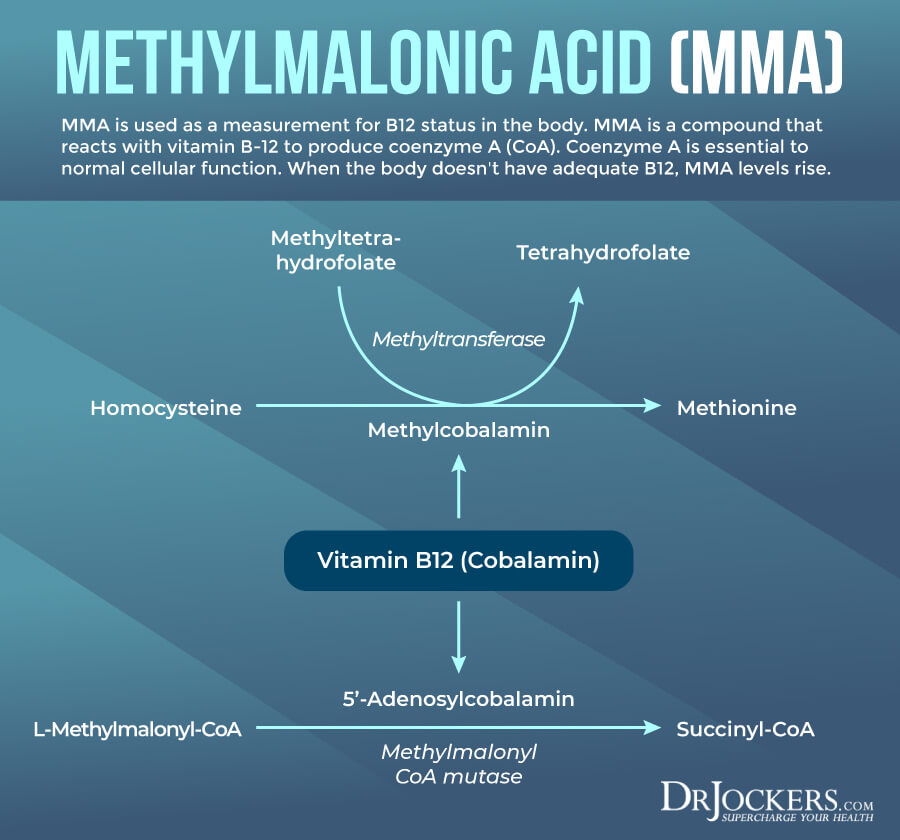
Methylmalonic Acid (MMA):
This is used as a measurement for B12 status in the body. Methylmalonic acid is a compound that reacts with vitamin B-12 to produce coenzyme A (CoA). Coenzyme A is essential to normal cellular function.
When the body doesn’t have adequate B12, MMA levels rise. This can even occur if there is plenty of B12 in the blood serum if it is not being properly utilized by the body. For this reason, the MMA test is more sensitive for B12 deficiency and metabolism problems than the serum B12 test. These tests are often used together but MMA is considered the most accurate test for B12 deficiency or B12 metabolism dysfunction (16).
Vitamin B12 is a critical part of the methylation process and is critical for proper hormone metabolism, neurotransmitter production, blood cell formation, cardiovascular and nervous system function among other things. Normal range for MMA is under 2.2 ug/mg.
Vitamin B6 Markers:
Vitamin B6 is critical for production of neurotransmitters and plays an important role in blood sugar stability and the development of the nervous system and immune system among other things. Use of medications, alcohol, tobacco smoke and exposure to pesticides and agricultural products can deplete vitamin B6 levels.
Some of the symptoms involved in B6 deficiency’s include changes in mood, such as irritability, anxiety and depression, confusion, muscle pains, low energy, or fatigue. Women with hormonal problems often present with low B6 levels.
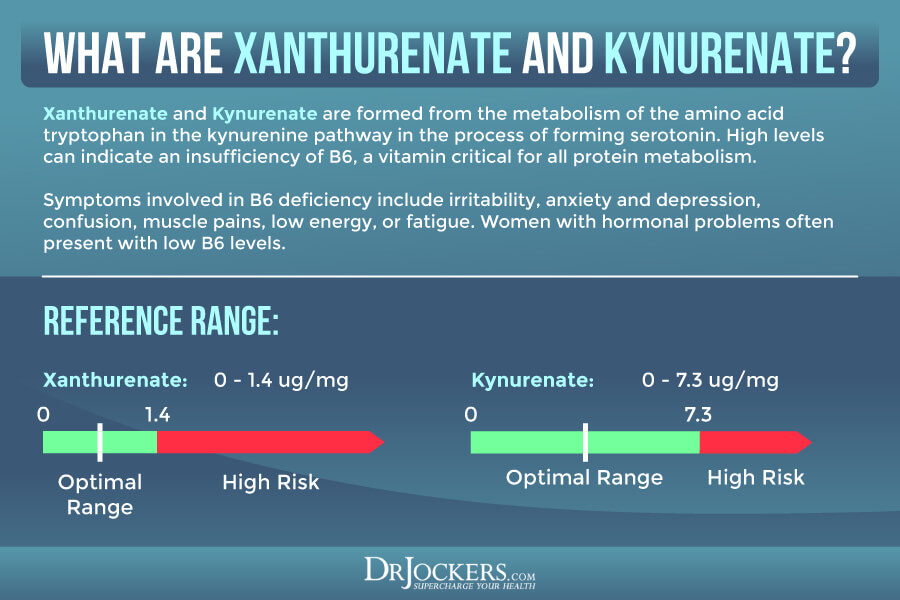
Xanthurenate is formed from the metabolism of the amino acid tryptophan in the kynurenine pathway in the process of forming serotonin. High levels can indicate an insufficiency of B6, a vitamin critical for all protein metabolism. Normal levels of xanthurenate on the DUTCH test are under 1.4 ug/mg.
High levels of cortisol and estrogen can also exacerbate xanthurenate elevations and increase the need for B6. High levels of xanthurenate form complexes that interfere with insulin and decrease insulin sensitivity.
Xanthurenate can also bind to iron and create a complex that increases DNA oxidative damage resulting in higher 8-OHdG levels. If both xanthurenate and 8-OHdG markers are elevated, there is likely an antioxidant insufficiency.
Kynurenate is another marker used for B6 deficiency. It is the product of the metabolism of tryptophon in the kynurenine pathway in the process of forming serotonin. With adequate B6, this is metabolized further but in cases of B6 deficiency high levels accumulate. High levels can increase pain and cause poor brain function. Normal levels on the DUTCH test should be under 7.3 ug/mg.
Glutathione Marker:
Pyroglutamate (or Pyroglutamic acid) is an intermediate in the glutathione metabolism and a marker of glutathione deficiency. Pyroglutamate is a step in the production/recycling of glutathione.
Glutathione is one of the most potent antioxidants in the human body. It is especially important in getting rid of toxins, including the harmful metabolites of estrogen detoxification 4-OH-E1 and 4-OH-E2. In healthy individuals, a very modest amount of Pyroglutamate is spilled in the urine. The normal range on the DUTCH test is 32–60 ug/mg.
If there is little glutathione available to be recycled, pyroglutamate will be low. Low values may indicate glutathione deficiency due to oxidative stress or chemical exposure. Supplementation with reduced glutathione, N-acetyl L-cysteine, lipoic acid, liposomal or acetylated glutathione and vitamin C (buffered) can raise glutathione levels.

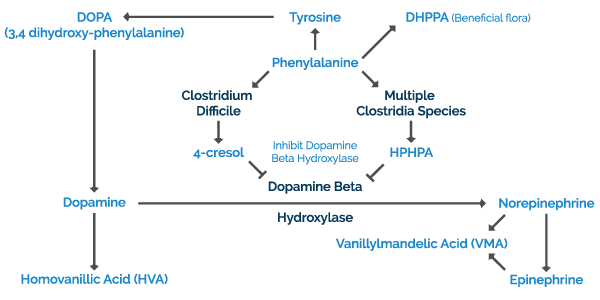
Neurotransmitter Metabolites:
Homovanillate (HVA) is a dopamine metabolite. When this compound is are low, it indicates your body is not making enough of these neurotransmitters. Low homovanillate indicates low levels of dopamine. The normal range on the DUTCH test is 4–13 ug/mg.
Symptoms associated with this condition are depression, sleep disturbances, inability to deal with stress, and fatigue. Some of the causes for low dopamine include chronic stress, trauma, chronic infections such as Clostridium Difficile, chronic inflammation, impaired methylation, low amino acid precursors and vitamin/mineral cofactors such as B2, B3, B6, Mg and Iron.
Vanilmandelate (VMA) is a metabolite of epinephrine and norepinephrine. It is often elevated due to acute stress increasing catecholamine output from the adrenal gland or from lead toxicity. The normal range on the DUTCH test is 2.4–6.4 ug/mg. Low levels are typically related to chronic stress, trauma, chronic inflammation, impaired methylation and low magnesium, vitamin C or copper.
Elevations of homovanillate and vanilmandelate indicate an over-activation of nervous system function involving these neurotransmitters. This can be for various reasons, but is most commonly associated with chronic stress or environmental toxin exposure.
Oxidative Stress Marker
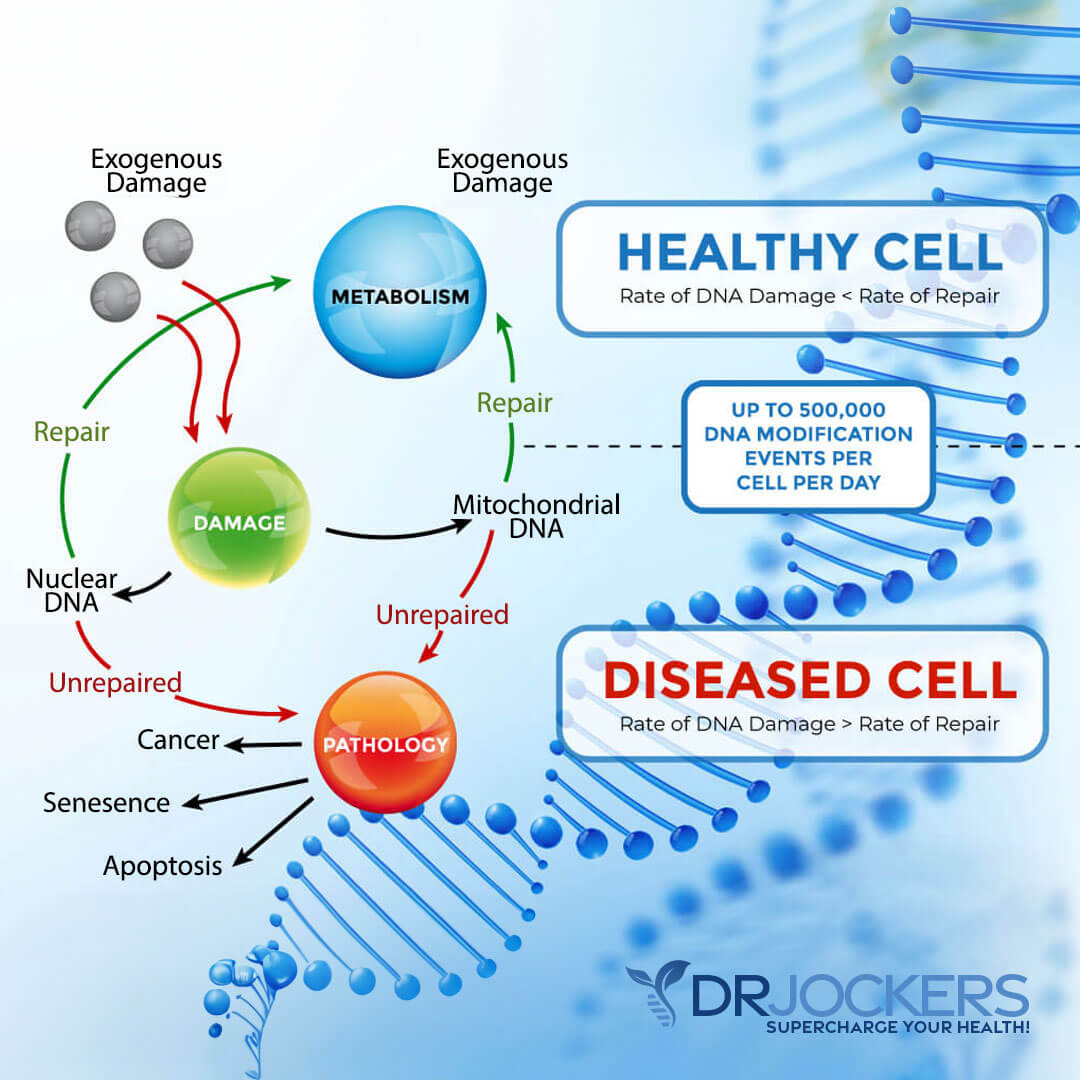
8-Hydroxy-2-Deoxyguanosine (8-OHdG) is a biomarker for oxidative stress that particularly measures the effect of endogenous oxidative damage to DNA. The marker is used to estimate the risk for various cancers and degenerative diseases and is associated with high cortisol, high blood pressure, diabetes, autoimmune diseases, fatty liver disease and more (17, 18).
8-OHdG is also used to estimate the DNA damage in humans after exposure to cancer-causing agents, such as tobacco smoke, asbestos fibers, heavy metals, and polycyclic aromatic hydrocarbons (19).
When local antioxidant systems fail, oxidative damage permanently occurs to lipids of cellular membranes, proteins, and DNA. In nuclear and mitochondrial DNA, 8-OHdG is predominantly formed due to free radical-induced oxidative (pro-mutative) lesions. Normal levels on the DUTCH test are under 5.2 ng/mg but we like to see it under 2.5 ng/mg for optimal health.
Conclusion:
If you are suffering from any of the symptoms stated in this article, chances are you need to get your hormones properly tested. We recommend getting the DUTCH Comprehensive Hormonal Analysis which is the most thorough and accurate way to test cortisol metabolism and sex hormone metabolism.
Once you receive the results of the DUTCH test it is even more important to have the results interpreted by someone who has experience dealing with patients suffering and the know how to decipher where the breakdown is in the hormonal pathway and what is necessary to help the body fix the breakdown.
If you want to work with a functional health coach to analyze your DUTCH test, I recommend this article with tips on how to find a great coach. On our website, we offer long-distance functional health coaching programs. For further support with your health goals, just reach out and our fantastic coaches are here to support your journey.

Inflammation Crushing Ebundle
The Inflammation Crushing Ebundle is designed to help you improve your brain, liver, immune system and discover the healing strategies, foods and recipes to burn fat, reduce inflammation and Thrive in Life!
As a doctor of natural medicine, I have spent the past 20 years studying the best healing strategies and worked with hundreds of coaching clients, helping them overcome chronic health conditions and optimize their overall health.
In our Inflammation Crushing Ebundle, I have put together my very best strategies to reduce inflammation and optimize your healing potential. Take a look at what you will get inside these valuable guides below!
Sources For This Article Include:
1. Herman JP, McKlveen JM, Ghosal S, et al. Regulation of the Hypothalamic-Pituitary-Adrenocortical Stress Response. Compr Physiol. 2016;6(2):603-621. Published 2016 Mar 15. PMCID: PMC4867107
2. Lee DY, Kim E, Choi MH. Technical and clinical aspects of cortisol as a biochemical marker of chronic stress. BMB Rep. 2015;48(4):209-216. PMCID: PMC4436856
3. Toufexis D, Rivarola MA, Lara H, Viau V. Stress and the reproductive axis. J Neuroendocrinol. 2014;26(9):573-586. PMCID: PMC4166402
4. Oyola MG, Handa RJ. Hypothalamic-pituitary-adrenal and hypothalamic-pituitary-gonadal axes: sex differences in regulation of stress responsivity. Stress. 2017;20(5):476-494. PMID: 28859530
5. Chong LS, Thai M, Cullen KR, Lim KO, Klimes-Dougan B. Cortisol Awakening Response, Internalizing Symptoms, and Life Satisfaction in Emerging Adults. Int J Mol Sci. 2017;18(12):2501. Published 2017 Nov 27. PMCID: PMC5751104
6. Dedovic K, Ngiam J. The cortisol awakening response and major depression: examining the evidence. Neuropsychiatr Dis Treat. 2015;11:1181-1189. Published 2015 May 14. PMCID: PMC4437603
7. Pulopulos MM, Hidalgo V, Puig-Perez S, Salvador A. Cortisol awakening response and cognitive performance in hypertensive and normotensive older people. Horm Behav. 2016;83:75-82. PMID: 27208824
8. Vallée M. Neurosteroids and potential therapeutics: Focus on pregnenolone. J Steroid Biochem Mol Biol. 2016;160:78-87. PMID: 26433186
9. Cable JK, Grider MH. Physiology, Progesterone. [Updated 2021 May 9]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan-. Link Here
10. Oettel M, Mukhopadhyay AK. Progesterone: the forgotten hormone in men?. Aging Male. 2004;7(3):236-257. PMID: 15669543
11. Doldi N, Gessi A, Destefani A, Calzi F, Ferrari A. Polycystic ovary syndrome: anomalies in progesterone production. Hum Reprod. 1998;13(2):290-293. PMID: 9557824
12. Esposito E, Cuzzocrea S. Antiinflammatory activity of melatonin in central nervous system. Curr Neuropharmacol. 2010;8(3):228-242. PMCID: PMC3001216
13. Tarocco, A., Caroccia, N., Morciano, G. et al. Melatonin as a master regulator of cell death and inflammation: molecular mechanisms and clinical implications for newborn care. Cell Death Dis 10, 317 (2019). Link Here
14. Escames G, López A, García JA, et al. The role of mitochondria in brain aging and the effects of melatonin. Curr Neuropharmacol. 2010;8(3):182-193. PMCID: PMC3001212
15. Reiter RJ, Manchester LC, Tan DX. Neurotoxins: free radical mechanisms and melatonin protection. Curr Neuropharmacol. 2010;8(3):194-210. PMCID: PMC3001213
16. Riphagen IJ, Minović I, Groothof D, et al. Methylmalonic acid, vitamin B12, renal function, and risk of all-cause mortality in the general population: results from the prospective Lifelines-MINUTHE study. BMC Med. 2020;18(1):380. Published 2020 Dec 10. PMID: 33298054
17. Valavanidis A, Vlachogianni T, Fiotakis C. 8-hydroxy-2′ -deoxyguanosine (8-OHdG): A critical biomarker of oxidative stress and carcinogenesis. J Environ Sci Health C Environ Carcinog Ecotoxicol Rev. 2009;27(2):120-139. PMID: 19412858
18. Graille M, Wild P, Sauvain JJ, Hemmendinger M, Guseva Canu I, Hopf NB. Urinary 8-OHdG as a Biomarker for Oxidative Stress: A Systematic Literature Review and Meta-Analysis. Int J Mol Sci. 2020;21(11):3743. Published 2020 May 26. PMID: 32466448
19. Prabhulkar S, Li CZ. Assessment of oxidative DNA damage and repair at single cellular level via real-time monitoring of 8-OHdG biomarker. Biosens Bioelectron. 2010;26(4):1743-1749. PMID: 20863679

Hi, great article! What is the cost of the comprehensive Dutch test? Thanks!
Hello Lisa, you can find that here: https://drjockers.com/the-dutch-complete-hormone-panel/