
Measuring Your Risk of Developing Heart Disease:
Heart disease is the leading cause of preventable death in the United States. Scientists are now saying that 95% of these heart disease related deaths are caused by cellular inflammation. Today’s technology allows us to analyze our level of cardiovascular inflammation and our risk of developing heart disease.
Inflammation is driven by several different routes in our body. Oxidative stress from excessive free radical formation and/or a deficiency in antioxidants is a common mechanism. Increased sympathetic stress response within the body causing catecholamine overload and burnout plays a role in most inflammatory cycles (1, 2, 3).
Finally, improper cell signaling due to excessive pro-inflammatory prostaglandin formation and immunological cytokine reactions is a staple ingredient in the inflammatory soup.

Tests to Analyze Inflammatory Levels:
When it comes to cardiovascular health, lipid panels are archaic and scientists have demonstrated that these tests have many limitations and only identify 40% of those at risk for coronary heart disease. People drop dead everyday with “normal” cholesterol levels, “normal” blood pressure and “normal” EKG findings.
Scientists have found much more advanced blood tests that can far more accurately assess your risk of heart disease. Three great tests that analyze the risk of inflammation in the coronary arteries include C Reactive Protein, Homocysteine, and Lipoprotein (a).
We include all of these key tests and more in our CardioPower Testing here I recommend this test to all my clients with a family or past history of heart disease.
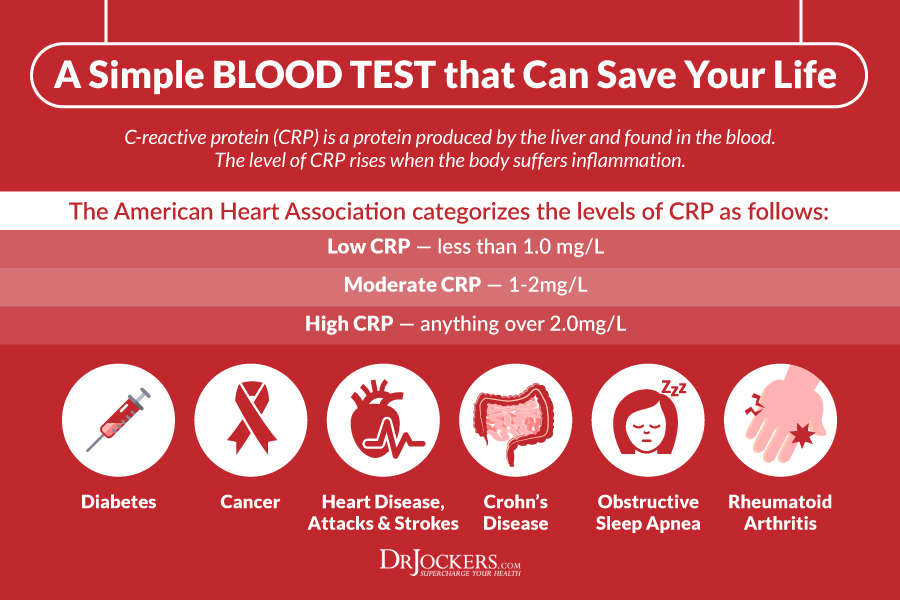
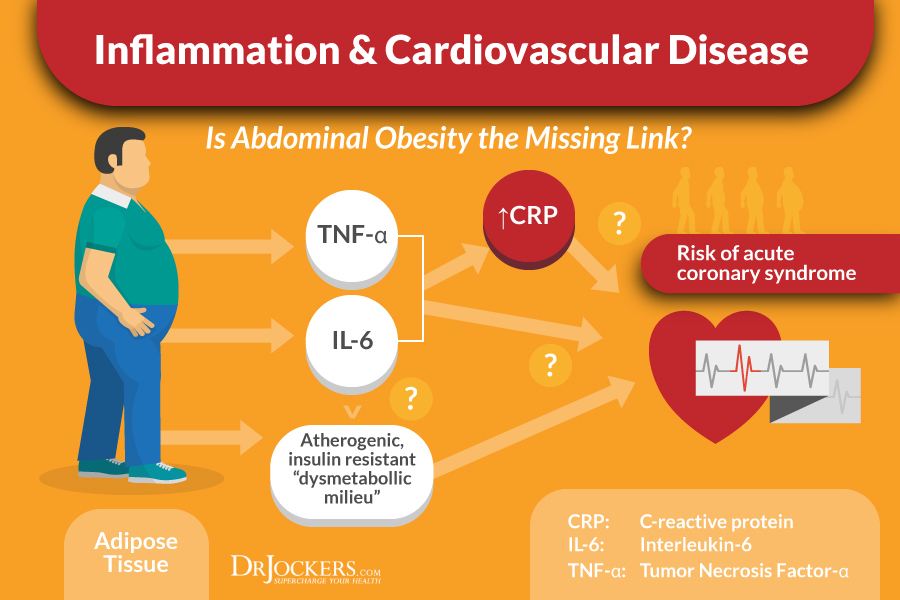
C Reactive Protein (CRP):
This is a protein found in the blood that rises in response to inflammation. During times of acute infections and resulting inflammatory responses CRP can elevate up to 50 times higher than normal. When the artery walls are inflamed and damaged CRP remains elevated (4, 5).
Even though many causative factors can increase CRP, research has shown that laboratory test level above 2.4 mg/l are at much higher risk of a heart attack compared to levels below 1 mg/l (6).
An anti-inflammatory diet and lifestyle are the critical keys to reducing CRP levels. This begins with a diet rich in phytonutrient dense vegetables, healthy fat and clean protein sources. Healthy fat sources include coconut products, avocados, olive oil, nuts, seeds, & purified omega-3 fish oil supplements.
Healthy protein includes wild-caught fish, grass-fed red meat and free range chicken, turkey and eggs. Anti-inflammatory herbs such as turmeric, cinnamon, ginger, rosemary, oregano & garlic are also powerful aids.
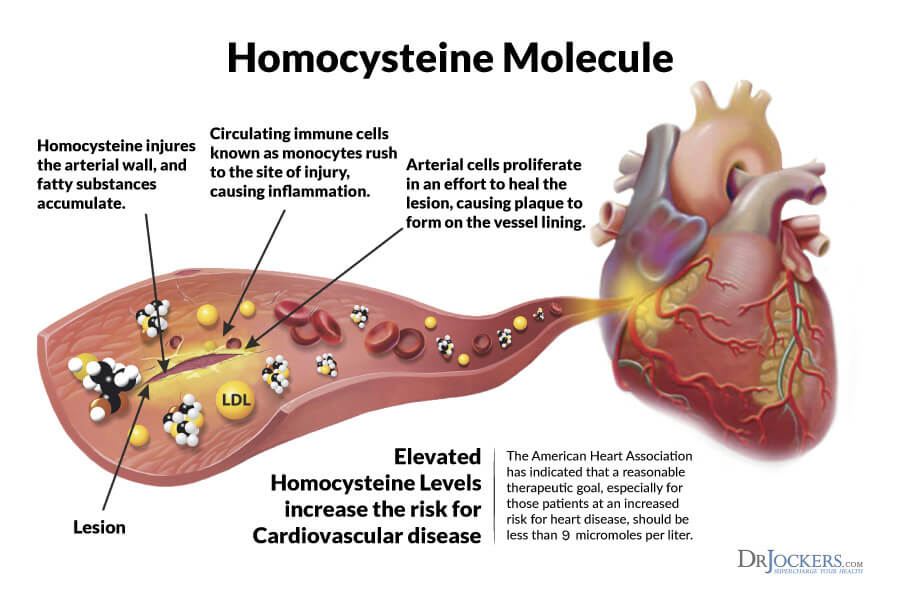
Homocysteine and Developing Heart Disease:
Homocysteine is an inflammatory amino acid that is produced as a byproduct of protein metabolism. Homocysteine-induced injury to the arterial wall is one of the factors that can initiate the process of atherosclerosis, leading to endothelial dysfunction and eventually to heart attacks and stroke (7, 8).
The amino acid methionine is digested and metabolized into homocysteine. When the body is sufficient in Vitamin B12, B6 & folate, excess homocysteine is remethylated into methionine or transsulfurated through vitamin B6 (9).
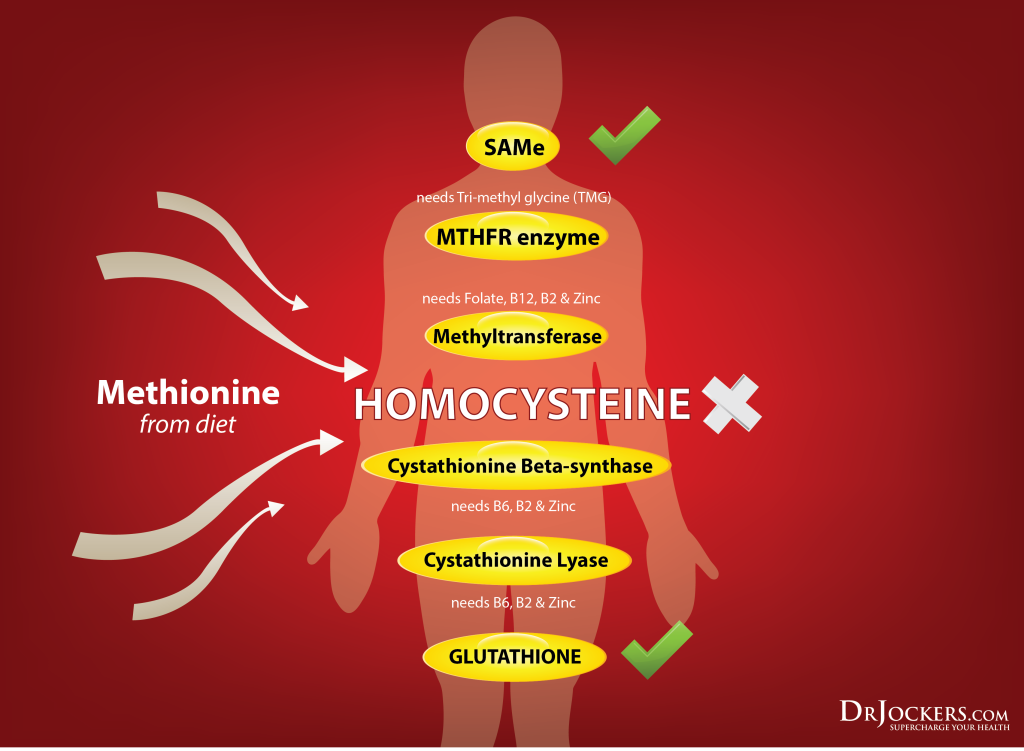
B Vitamins and Homocysteine:
When the body is deficient in any of these key B vitamins, it is unable to remethylate or transsulfurate the homocysteine. This leads to elevated levels of this inflammatory agent in the blood (10). Blood tests that show homocysteine levels above 6.3 umol/L are an indication of methylation deficiencies and elevated risk of heart disease (11).
Many individuals that have the MTHFR gene polymorphyism and other single nucleotide polymorphisms (SNP’s) have trouble with the methylation process and often have elevated homocysteine levels. To address this, one could try to juice green veggies and beets on a regular basis to get large amounts of these B vitamins and methylation elements.
Supplementing with premethylated forms of B2, B6, B12, and trimethylglycine have been shown to significantly lower homocysteine levels. Adequate amounts of magnesium, zinc and cellular anti-oxidants are also critical players in homocysteine metabolism (12). Clinically, I use Methyl Power as a main supplement to help reduce homocysteine levels.

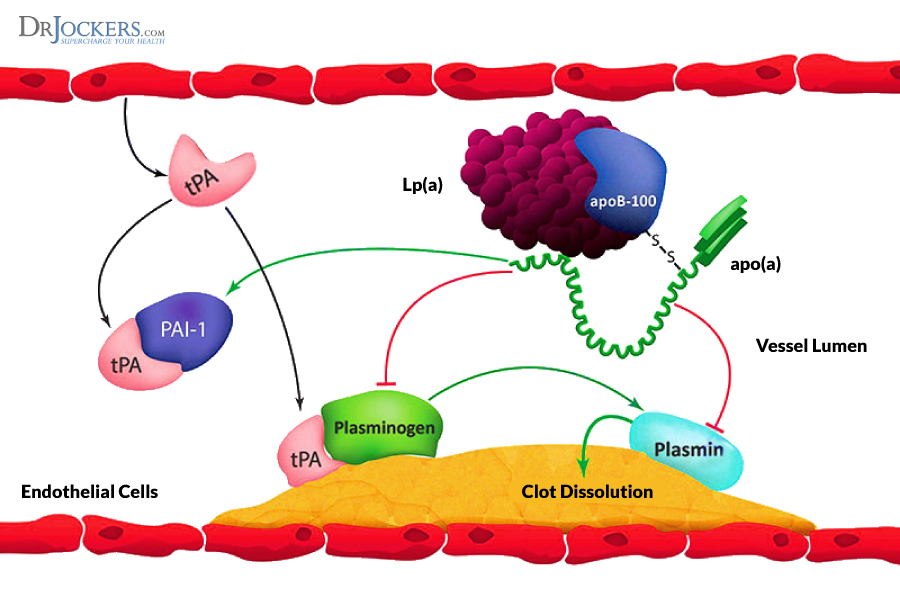
Lipoprotein (a) Levels and Developing Heart Disease:
Lipoprotein (a) is a particular subclass of LDL cholesterol. Lp (a) is very similar in structure to a critical enzyme called plasminogen (13). Plasminogen helps the body dissolve blood clots. At any one time, our bodies are constantly making and dissolving microscopic blood clots. This dance is very delicate and dependent on a healthy balance of two blood clotting systems and this balance is key to know for your risk of developing heart disease.
If Lp(a) competes for binding spots for this blood clot dissolver, the blood system balance may form blood clots. The majority of heart attacks are caused by a blood clot in a heart artery at a site of atherosclerosis. Lp(a) has been shown to stimulate our immune cells to deposit cholesterol into heart artery walls thereby promoting the development of atherosclerosis (14).
A Lp(a) levels should be under 20 mg/dl and ideally under 14 mg/dl. This is an important test to consider when it comes to developing heart disease.
Lower Lipoprotein Levels:
Several nutritional supplements have been shown to lower Lp(a) naturally. High doses of vitamin B3 or Niacin is the most effective way to bring down Lp(a) levels (16, 17). The challenge with high doses of niacin is that it causes annoying hot flushes where the face and neck get red and the individual feels very warm.
This is quite scary for the individual if they are not educated on the flush beforehand and most doctors do not understand that this is a normal phenomenon.
Other key supplements include CoQ10, N Acetyl Cysteine, Acetyl-L-carnitine and alpha lipoic acid to boost mitochondrial health (18, 19, 20, 21). I put my clients with elevated Lp (a) on Mito Support which contains clinical verified dosages of these mitochondrial enhancing nutrients.

Sources For This Article Include:
1. Osiecki H. The role of chronic inflammation in cardiovascular disease and its regulation by nutrients. Altern Med Rev. 2004 Mar;9(1):32-53. PMID: 15005643
2. Li JJ, Chen JL. Inflammation may be a bridge connecting hypertension and atherosclerosis. Med Hypotheses. 2005;64(5):925-9. PMID: 15780486
3. Virdis A, Schiffrin EL. Vascular inflammation: a role in vascular disease in hypertension? Curr Opin Nephrol Hypertens. 2003 Mar;12(2):181-7. PMID: 12589179
4. Ridker PM. Inflammation, High-Sensitivity C-Reactive Protein, and Vascular Protection. Texas Heart Institute Journal. 2010;37(1):40-41.
5. Maksimowicz-McKinnon K, Bhatt DL, Calabrese LH. Recent advances in vascular inflammation: C-reactive protein and other inflammatory biomarkers. Curr Opin Rheumatol. 2004 Jan;16(1):18-24. PMID: 14673384
6. Ridker PM. C-Reactive Protein, Inflammation, and Cardiovascular Disease: Clinical Update. Texas Heart Institute Journal. 2005;32(3):384-386.
7. McCully KS. Homocysteine and the pathogenesis of atherosclerosis. Expert Rev Clin Pharmacol. 2015 Mar;8(2):211-9. PMID: 25653125
8. Hankey GJ, Eikelboom JW. Homocysteine and stroke. Curr Opin Neurol. 2001 Feb;14(1):95-102. PMID: 11176224
9. Mandaviya PR, Stolk L, Heil SG. Homocysteine and DNA methylation: a review of animal and human literature. Mol Genet Metab. 2014 Dec;113(4):243-52. PMID: 25456744
10. McMullin MF, Young PB, Bailie KE, Savage GA, Lappin TR, White R. Homocysteine and methylmalonic acid as indicators of folate and vitamin B12 deficiency in pregnancy. Clin Lab Haematol. 2001 Jun;23(3):161-5. PMID: 11553056
11. Sadeghian S, Fallahi F, Salarifar M, Davoodi G, Mahmoodian M, Fallah N, Darvish S, Karimi A; Tehran Heart Center. Homocysteine, vitamin B12 and folate levels in premature coronary artery disease. BMC Cardiovasc Disord. 2006 Sep 26;6:38. PMID: 17002799
12. Ueland PM, Holm PI, Hustad S. Betaine: a key modulator of one-carbon metabolism and homocysteine status. Clin Chem Lab Med. 2005;43(10):1069-75. PMID: 16197300
13. Dubé JB, Boffa MB, Hegele RA, Koschinsky ML. Lipoprotein(a): more interesting than ever after 50 years. Curr Opin Lipidol. 2012 Apr;23(2):133-40. PMID: 22327610
14. Nordestgaard BG, Chapman MJ, Ray K, Borén J, Andreotti F, Watts GF, Ginsberg H, Amarenco P, Catapano A, Descamps OS, Fisher E, Kovanen PT, Kuivenhoven JA, Lesnik P, Masana L, Reiner Z, Taskinen MR, Tokgözoglu L, Tybjærg-Hansen A; European Atherosclerosis Society Consensus Panel. Lipoprotein(a) as a cardiovascular risk factor: current status. Eur Heart J. 2010 Dec;31(23):2844-53. PMID: 20965889
15. Emerging Risk Factors Collaboration, Di Angelantonio E, Gao P, Pennells L, Kaptoge S, Caslake M, Thompson A, Butterworth AS, Sarwar N, Wormser D, Saleheen D, Ballantyne CM, Psaty BM, Sundström J, Ridker PM, Nagel D, Gillum RF, Ford I, Ducimetiere P, Kiechl S, Koenig W, Dullaart RP, Assmann G, D’Agostino RB Sr, Dagenais GR, Cooper JA, Kromhout D, Onat A, Tipping RW, Gómez-de-la-Cámara A, Rosengren A, Sutherland SE, Gallacher J, Fowkes FG, Casiglia E, Hofman A, Salomaa V, Barrett-Connor E, Clarke R, Brunner E, Jukema JW, Simons LA, Sandhu M, Wareham NJ, Khaw KT, Kauhanen J, Salonen JT, Howard WJ, Nordestgaard BG, Wood AM, Thompson SG, Boekholdt SM, Sattar N, Packard C, Gudnason V, Danesh J. Lipid-related markers and cardiovascular disease prediction. JAMA. 2012 Jun 20;307(23):2499-506. PMID: 22797450
16. Pan J, Van JT, Chan E, Kesala RL, Lin M, Charles MA.Extended-release niacin treatment of the atherogenic lipid profile and lipoprotein(a) in diabetes. Metabolism. 2002 Sep;51(9):1120-7. PMID: 12200755
17. Pan J, Lin M, Kesala RL, Van J, Charles MA. Niacin treatment of the atherogenic lipid profile and Lp(a) in diabetes. Diabetes Obes Metab. 2002 Jul;4(4):255-61. PMID: 12099974
18. Singh RB, Niaz MA. Serum concentration of lipoprotein(a) decreases on treatment with hydrosoluble coenzyme Q10 in patients with coronary artery disease: discovery of a new role. Int J Cardiol. 1999 Jan;68(1):23-9. PMID: 10077397
19. Shojaei M, Djalali M, Khatami M, Siassi F, Eshraghian M. Effects of carnitine and coenzyme Q10 on lipid profile and serum levels of lipoprotein(a) in maintenance hemodialysis patients on statin therapy. Iran J Kidney Dis. 2011 Mar;5(2):114-8. PMID: 21368390
20. Harding SV, Rideout TC, Jones PJ. Evidence for using alpha-lipoic acid in reducing lipoprotein and inflammatory related atherosclerotic risk. J Diet Suppl. 2012 Jun;9(2):116-27. PMID: 22607646
21. Gavish D, Breslow JL. Lipoprotein(a) reduction by N-acetylcysteine. Lancet. 1991 Jan 26;337(8735):203-4. PMID: 1670844

Thanks for that article. I read another article recently:
https://www.naturalnews.com/043882_homocysteine_heart_disease_circulatory_system.html
where it says:
“How one develops high levels of homocysteine
Homocysteine is a metabolic byproduct of protein metabolism and in particular the metabolism of methionine. Methionine is found in meats, seafood, dairy products, eggs, sesame seeds and Brazil nuts.”
Does it mean that if one has elevated homocysteine levels one should avoid these foods?
Marek – I wrote that article on homocysteine in NaturalNews. No, individuals with high homocysteine do not necessarily need to avoid methionine containing foods…they need to increase their methylated B6, B2, methylfolate and methylcobalamin and anti-oxidants.
I have an opportunity at a nearby hospital to have a test they call Cardiac Scoring? Would this test be helpful in evaluating my heart health. thank you for all you do.
Utley – I had a calcium scoring test, it evaluates levels of calcified plaque (not good) in your arteries. Non-invasive test, very low radiation.